Introduction
Regarding the musculoskeletal system, the various muscles, tissues, and ligaments help protect the spine and vital organs that make the body functional. These muscles are sectioned into different groups that help provide movement and motion to the host without feeling pain. However, when normal factors or traumatic forces begin to affect the musculoskeletal system, it can cause unnecessary stress on the muscle fibers. These environmental factors can lead to muscle pain and correlating symptoms affecting the upper and lower body portions. When muscle pain affects the body, it can mask other pre-existing conditions that can make the individual feel miserable. Fortunately, many individuals will go to therapy treatment to reduce the effects of muscle pain and have a personalized plan that they can follow to prevent muscle pain from returning in the future. Today’s article focuses on one of the non-surgical treatments known as MET (muscle energy technique) therapy that can help reduce the effects of muscle pain and what is the protocol treatment plan to relieve muscle pain in the body. We work with certified medical providers who use our patients’ valuable information to treat individuals suffering from muscle pain while informing them about non-surgical treatments like MET therapy that can help reduce the effects of musculoskeletal pain. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
How Does Muscle Pain Affect The Body?
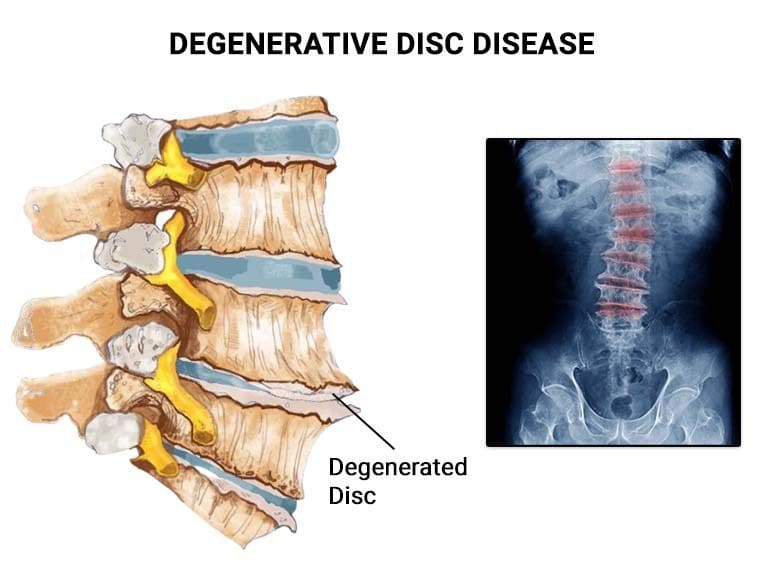
Do you experience muscle aches, stiffness, or pain in one or more parts of your body? These pain-like symptoms are often caused by muscle pain. Research studies revealed that free nerve endings in muscle fibers can send pain signals to the brain, leading to decreased productivity and economic burden. Overstretching muscles during daily routines can cause trigger points, small nodules in muscle fibers that cause stiffness and contraction. This can lead to misalignment and additional problems over time.

Muscle pain can be a symptom of different conditions, with severity ranging from acute to chronic. Research studies stated that when musculoskeletal pain affects more than 30% of the world, it can significantly impact an individual’s life. This type of pain can be related to sensory innervation of the bones, joints, and muscles and can negatively affect a person’s daily routine. However, there are various ways to reduce muscle pain, which individuals can incorporate to relieve muscle pain and reduce its chances of returning.
Movement As Medicine- Video

When it comes to musculoskeletal pain, it can have a significant impact on a person’s body. It can affect their daily routine, causing them to have limited mobility and feel miserable. Musculoskeletal pain causes the involved muscle fibers to stiffen up and contract. This causes the surrounding muscles to compensate for the pain the affected muscle feels and causes body misalignment. However, all is not lost, as available treatments can help reduce the effects of muscle pain and can bring back a person’s mobility. One of these treatments is MET (muscle energy technique) therapy. Research studies reveal that MET is an osteopathic technique that many pain specialists like chiropractors and massage therapists use to improve musculoskeletal function by mobilizing joints, stretching tight muscles and facia to reduce pain, and improving circulation and lymphatic flow. Since many individuals don’t stretch their bodies as often as needed, their muscles can become tight and stiff, which causes the development of muscle pain. So by utilizing MET therapy, a person dealing with muscle pain can regain mobility. MET therapy can also be combined with other treatments like chiropractic care to help realign the body out of subluxation and strengthen/lengthen tight muscles. The video above explains how movement is used as medicine to reduce the effects of muscle pain.
MET Treatment Protocol

According to “Clinical Application of Neuromuscular Techniques,” written by Leon Chaitow, N.D., D.O., and Judith Walker DeLany, L.M.T., when the body is experiencing restricted joints, incorporating MET therapy can indicate where the problem is located in the soft musculoskeletal tissues. When it comes to many individuals going to MET therapy for muscle pain, many doctors have their protocol approach when assessing patients for muscle pain treatment.
Looking At Body Language
When assessing patients with muscle pain, looking at their body language and how they carry themselves is important. Many doctors and pain specialists should note how the individual is breathing, their posture, and if there is any perspiration on the skin. By taking note of how the individual looks physically, many doctors will begin to formulate a treatment plan while communicating with the patient to gather more information and create a trusting relationship. Afterward, the doctor can start the physical examination to locate where the pain is in the body.
Physical Examination
The MET treatment protocol’s physical examination portion allows the doctor to go through a sequential assessment involving observation, joint and muscle testing, palpations, evaluation of accessory movement, etc., to create a basic formula to create a personalized treatment plan. The physical examination of MET allows the muscles to influence muscle contractions on the surrounding fascia and alter the muscle’s physiology by reflex mechanisms. These stretches help the restricted joints be re-mobilized, and help stretch the tightened muscles to feel relief from metabolic waste.
Therapeutic Plan
The therapeutic plan for MET treatment is personalized and customizable for the individual to follow through to reduce muscle pain from re-occurring in the body. Many doctors specializing in MET therapy work with other associated medical providers to ensure that the person in pain has the help they need. Physical therapy, dietary nutrition, non-surgical treatments, and health coaches all work together to create a personalized health and wellness plan to make sure that muscle pain and its associated factors are being treated. This allows individuals to be more mindful of their bodies and regain their health and wellness.
Conclusion
Muscle pain can affect a person’s ability to move around and can affect multiple areas in the upper and lower body portions. Muscle pain correlates to tight muscle fibers that become stiff and can develop trigger points in the fascia and cause restricted movement. When this happens, it can cause the individual to miss out on daily activities and prevent them from working. Luckily available treatments can help reduce muscle pain by re-mobilizing the joints and stretching out the tight muscle. MET, or muscle energy technique therapy, helps stretch muscle fascia and mobilize joints to regain the body’s range of motion and help reduce muscle pain. Many people who incorporate MET into their daily routine can restore mobility and continue their health and wellness journey.
References
Chaitow, L., & Delany, J. (2002). Clinical application of neuromuscular techniques. Vol. 2, The lower body. Churchill Livingstone.