Medical staff helping asian patient with neck brace removing cervical neck collar after injury accident during consultation.. Injured young adult healing fracture and trauma in hospital waiting area
“Individuals who have suffered cervical acceleration-deceleration/CAD more commonly known as whiplash, can experience headaches, and other symptoms like neck stiffness, pain, fatigue, and shoulder/neck/back discomfort. Can non-surgical and conservative treatments help alleviate the symptoms?”
Table of Contents
Cervical Acceleration – Deceleration or CAD
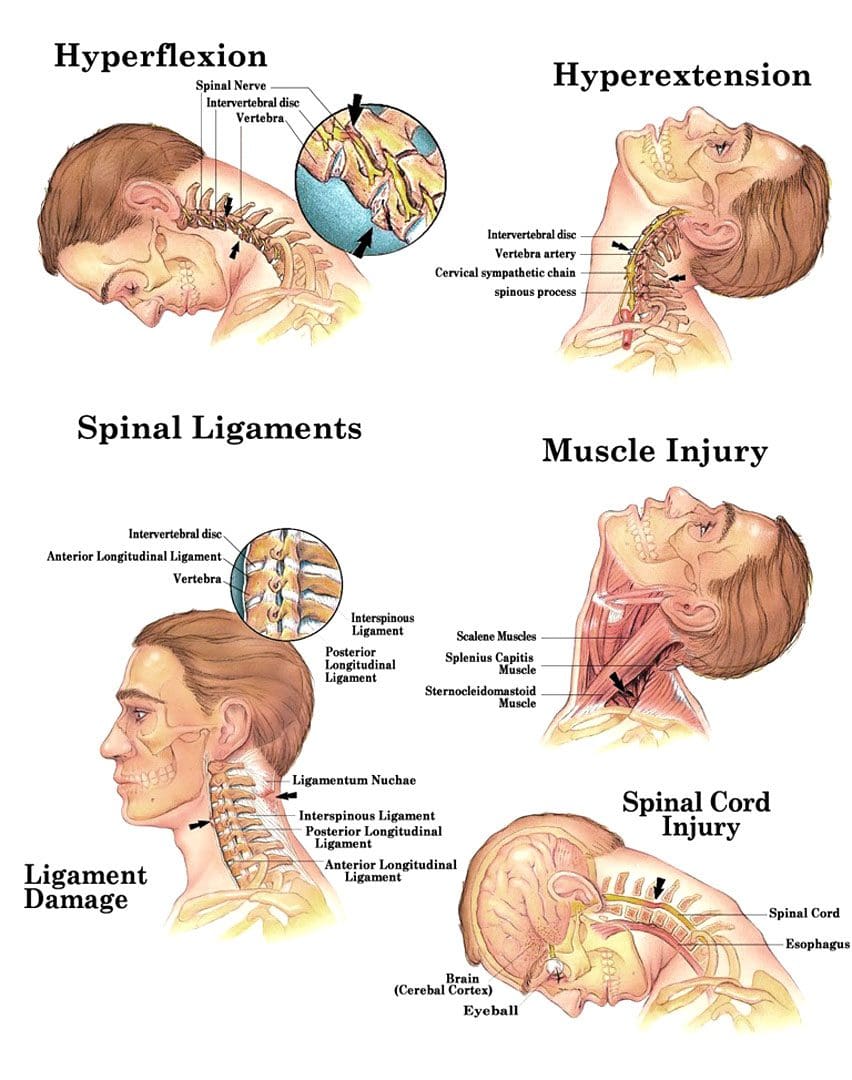
Cervical acceleration-deceleration is the mechanism of a neck injury caused by a forceful back-and-forth neck motion. It happens most commonly in rear-end vehicle collisions when the head and neck whip forward and backward with intense acceleration and/or deceleration causing the neck to flex and/or extend rapidly, more than normally, straining and possibly tearing muscle tissues and nerves, ligaments, dislocation of spinal discs and herniations, and cervical bone fractures.
For symptoms that do not improve or worsen after 2 to 3 weeks, see a healthcare provider or chiropractor for further evaluation and treatment.
Whiplash injuries strain or sprain the neck muscles and/or ligaments, but can also affect the vertebrae/bones, disc cushions between the vertebrae, and/or the nerves.
Whiplash symptoms can present right away, or after several hours to a few days after the incident, and tend to worsen in the days after the injury. Symptoms can last a few weeks to a few months, and can severely limit activity and range of motion. Symptoms can include: (National Institute of Neurological Disorders and Stroke. 2023)
Pain that extends into the shoulders and back.
Neck stiffness
Limited neck motion
Muscle spasms
Numbness and tingling sensations – paresthesias or pins and needles in the fingers, hands, or arms.
Headaches – A whiplash headache usually starts at the base of the skull and can vary in intensity. Most individuals experience pain on one side of the head and toward the back, though some can experience symptoms all over their head, and a small number experience headaches on the forehead or behind the eyes. (Monica Drottning. 2003)
The headaches can become aggravated by moving the neck around, especially when looking up.
Headaches are often associated with shoulder pain along with sensitive neck and shoulder muscles that when touched can increase pain levels.
Whiplash headaches can lead to chronic neck-related headaches known as cervicogenic headaches. (Phil Page. 2011)
It is also important to rest your neck area following the injury.
A cervical collar can be utilized temporarily to stabilize the neck, but for long-term recovery, it is recommended to keep the area mobile.
Physical activity reduction until the individual can look over both shoulders, and tilt their head all the way forward, all the way back, and from side to side without pain or stiffness.
Non-steroidal anti-inflammatories – NSAIDs – Ibuprofen or Naproxen.
Muscle relaxers
If symptoms do not improve, a healthcare provider may recommend physical therapy and/or stronger pain medications. For whiplash headaches that last for several months, acupuncture, or spinal injections may be recommended.
Neck Injuries
References
National Institute of Neurological Disorders and Stroke. Whiplash Information Page.
Drottning M. (2003). Cervicogenic headache after a whiplash injury. Current pain and headache reports, 7(5), 384–386. doi.org/10.1007/s11916-003-0038-9
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
Can lumbar traction therapy alleviate an individual’s lower back pain by restoring weak trunk muscles over time?
Table of Contents
Introduction
The trunk muscles are the body’s main stabilizers that support upper body weight and stabilize the lower body weight. These muscles work with the lumbar back muscles so the individual can maintain good posture and be mobile when in motion without pain. However, when traumatic or normal forces start to affect the trunk muscles, it can lead to unwanted musculoskeletal pain that can lead to a life of disability and affect their performance in their routine. Weak truck muscles can lead to low back pain issues while causing referred pain to the lower extremities. However, many individuals are finding ways to strengthen their trunk muscles by slowly integrating core exercises and going to non-surgical treatments to reduce the pain they have been experiencing. Today’s article looks at how weak truck muscles correlate with low back pain and how non-surgical treatments like lumbar traction can reduce pain associated with weak trunk muscles. Additionally, we communicate with certified medical providers who incorporate our patients’ information to ease low back pain associated with weak trunk muscles, causing many musculoskeletal issues in the lower body. We also inform them that non-surgical treatments can help re-strengthen the truck muscles. We encourage our patients to ask amazing educational questions for our associated medical providers about their symptoms correlating with weak trunk muscles. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer
Weak Trunk Muscles Correlate With Low Back Pain
Do you often experience low back pain after carrying a heavy object from one location to another at work? Do you slouch more than usual when you are relaxing at home? Or have you noticed that you can’t hold a plank for less than 30 seconds during a workout? Many individuals dealing with these issues in these scenarios could be dealing with weak core muscles that can lead to low back pain. Since low back pain is a common problem that many people have, some of the correlating factors could be weak trunk muscles. Weak trunk muscles in the body can be due to the body naturally degenerating, causing the intervertebral disc to deteriorate. When the water content and spinal disc height begin to go through mechanical changes from unwanted pressure loads, it can cause the intervertebral discs to bulge out of the spine more and cause the surrounding ligaments and muscles to deal with more stress and become weak over time. (Adams et al., 1990) When the trunk muscles weaken, the lower extremities will start to develop musculoskeletal conditions that can lead to pain. Spinal disorders develop over time when normal or traumatic forces begin to affect the quality and quantity of the trunk muscle functions for its range of motion, strength, and endurance when a person is doing normal activities. (Allen, 1988)
So how would weak trunk muscles and low back pain have this relationship to affect a person’s spine? When muscle activity begins to be reduced within the trunk region, symptoms like stiffness and pain can cause postural shrinkage to the spinal disc in the lumbar region. (Cholewicki, 2004) Additionally, when dealing with low back pain, their trunk muscles undergo structural changes that can affect their stability. These changes can lead to reduced movement speed and range of motion, which then causes many of the accessory muscles to compensate for the pain that the person is experiencing. (Van Dieën, Cholewicki, & Radebold, 2003) However, numerous individuals will opt for a treatment plan to reduce low back pain and also help strengthen weak core muscles.
Can Core Exercises Help With Back Pain?-Video
When it comes to strengthening and restoring weak muscles to reduce low back pain, many individuals will try exercising to lessen the pain they are experiencing in their lumbar spine and strengthen their weakened core muscles. The video above indicates that including core strengthening workouts in a workout routine can be essential to pain management. Exercising alone can be challenging without the right motivation, but it can be included in a personalized treatment plan that can be effective and customizable to manage lumbar impairment. (Li & Bombardier, 2001) Many individuals opt for non-surgical treatments due to their cost-effectiveness and how safe it is on the spine to reduce muscle weakness within the trunk muscles.
Lumbar Traction Restoring Weak Trunk Muscles
When dealing with weak trunk muscles correlating with low back pain, incorporating non-surgical treatment could be the answer to reducing the pain they have been experiencing. Non-surgical treatments like lumbar traction, spinal decompression, massage therapy, physical therapy, and chiropractic care utilize mechanical and manual techniques to reduce pain in the upper and lower body portions, help stretch out shortened and tight muscles, and kick-start the body’s natural healing process. Since lumbar traction is a non-surgical treatment, it can help restore muscle strength within the trunk region. Lumbar traction can be used manually or mechanically to increase intervertebral disc space, decrease mechanical stress, and reduce muscle spasms. (Wegner et al., 2013) When many individuals feel relief from their pain and strengthen their trunk muscles gradually, they will notice a difference in their routine and continue to be pain-free after a few session treatments.
References
Adams, M. A., Dolan, P., Hutton, W. C., & Porter, R. W. (1990). Diurnal changes in spinal mechanics and their clinical significance. J Bone Joint Surg Br, 72(2), 266-270. doi.org/10.1302/0301-620X.72B2.2138156
Allen, M. E. (1988). Clinical kinesiology: measurement techniques for spinal disorders. Orthop Rev, 17(11), 1097-1104. www.ncbi.nlm.nih.gov/pubmed/3205587
Cholewicki, J. (2004). The effects of lumbosacral orthoses on spine stability: what changes in EMG can be expected? J Orthop Res, 22(5), 1150-1155. doi.org/10.1016/j.orthres.2004.01.009
Li, L. C., & Bombardier, C. (2001). Physical therapy management of low back pain: an exploratory survey of therapist approaches. Phys Ther, 81(4), 1018-1028. www.ncbi.nlm.nih.gov/pubmed/11276184
Van Dieën, J. H., Cholewicki, J., & Radebold, A. (2003). Trunk Muscle Recruitment Patterns in Patients With Low Back Pain Enhance the Stability of the Lumbar Spine. Spine, 28(8), 834-841. doi.org/10.1097/01.brs.0000058939.51147.55
Wegner, I., Widyahening, I. S., van Tulder, M. W., Blomberg, S. E., de Vet, H. C., Bronfort, G., Bouter, L. M., & van der Heijden, G. J. (2013). Traction for low-back pain with or without sciatica. Cochrane Database Syst Rev, 2013(8), CD003010. doi.org/10.1002/14651858.CD003010.pub5
Various kind of bread, such as wholegrain, rice crakers, crispbreads and different nut butter, such as peanut, crunchy cashew and almond butter
For individuals with peanut allergies, can finding a peanut alternative be as satisfying as a real creamy or crunchy peanut butter sandwich?
Table of Contents
Peanut Butter Sandwich Alternatives
For individuals who are unable to have a peanut butter sandwich due to an allergy, there are healthy satisfying alternatives. Tree nut butter, seed butter, and deli meats can all satisfy sandwich cravings and provide nutrition. Here are a few healthy, nutritious alternatives to try out:
Sunflower Seed Butter and Jam, Jelly, or Preserves
It can be substituted for a PBJ with jam, jelly, and preserves.
Ham and Cheese, Grainy Mustard on Rye Bread
Getting ham and cheese from the deli can potentially have cross-contamination with allergens during slicing and packaging.
Prepackaged and sliced ham and cheese is a safer bet in terms of allergens.
It is recommended to read the ingredient label for potential allergens, as processing in facilities can have cross-contamination issues. (William J. Sheehan, et al., 2018)
Turkey, Tomato, Lettuce, and Hummus on Whole Grain Bread
The same is true for turkey and is recommended to buy prepackaged and sliced.
Check the ingredients for possible allergens.
Hummus is made from chickpeas/garbanzo beans and tahini/ground sesame seeds.
Hummus comes in a variety of flavors that can be used as a dip or spread.
Although chick peas’ are a member of the legume family, hummus can be tolerated with peanut allergies. (Mathias Cousin, et al., 2017)
Check with a healthcare provider if unsure.
Pita Pocket with Salad and Hummus
Pita pockets are great with hummus stuffed with vegetables.
This is a delicious crunchy pocket sandwich loaded with protein, fiber vitamins, and minerals.
Cashew butter on a hot English muffin with raisins on top for a boost of iron is reminiscent of a cinnamon roll.
Pumpkin Seed Butter and Honey Sandwich
Pumpkin butter is made from the orange flesh of the pumpkin.
Pumpkin seed butter is made by roasting pumpkin seeds and grinding them to a butter consistency.
The seed butter can be spread on bread and drizzled with some honey on top for a nutritious and delicious snack.
There are tasty healthy peanut butter alternatives that can be mixed, matched, and reinvented into various satisfying sandwiches. Individuals are recommended to consult their healthcare provider or a dietician or nutritionist to find what works for them.
Smart Choices, Better Health
References
Lavine, E., & Ben-Shoshan, M. (2015). Allergy to sunflower seed and sunflower butter as a proposed vehicle for sensitization. Allergy, asthma, and clinical immunology: Official Journal of the Canadian Society of Allergy and Clinical Immunology, 11(1), 2. doi.org/10.1186/s13223-014-0065-6
U.S. Department of Agriculture: FoodData Central. Seeds, sunflower seed butter, with salt added (Includes foods for USDA’s Food Distribution Program).
Sheehan, W. J., Taylor, S. L., Phipatanakul, W., & Brough, H. A. (2018). Environmental Food Exposure: What Is the Risk of Clinical Reactivity From Cross-Contact and What Is the Risk of Sensitization. The journal of allergy and clinical immunology. In practice, 6(6), 1825–1832. doi.org/10.1016/j.jaip.2018.08.001
Gorrepati, K., Balasubramanian, S., & Chandra, P. (2015). Plant-based butters. Journal of food science and technology, 52(7), 3965–3976. doi.org/10.1007/s13197-014-1572-7
Cousin, M., Verdun, S., Seynave, M., Vilain, A. C., Lansiaux, A., Decoster, A., & Sauvage, C. (2017). Phenotypical characterization of peanut-allergic children with differences in cross-allergy to tree nuts and other legumes. Pediatric allergy and immunology: Official publication of the European Society of Pediatric Allergy and Immunology, 28(3), 245–250. doi.org/10.1111/pai.12698
Almond Board of California. Nutrient comparison chart for tree nuts.
American Academy of Allergy, Asthma and Immunology. Everything you need to know about a tree nut allergy.
How does innovated non-surgical treatment help assist individuals with cervical spinal pain to reduce headaches?
Table of Contents
Introduction
Do you or your loved ones often experience headaches that don’t disappear? Do you often feel your shoulder and neck muscles ache after looking down at your cell phone? Or do you feel aches after being slouched for an extended period? Many of these scenarios correlate with referred pain in the cervical spinal region, which can develop into neck pain. The neck region is located in the upper body portion and provides mobility for the head without pain and discomfort. The neck region also has surrounding muscles and ligaments that support the spine and protects the thyroid and spinal cord. However, just like the back region, it is susceptible to pain as many individuals can overstretch the neck muscles, and it can cause referred pain to the shoulders and head, leading to pain-like symptoms that can lead to a life of disability. However, non-surgical treatments can minimize the pain and help strengthen the surrounding muscles in the neck region. Today’s article focuses on how cervical spinal pain connects with headaches and how decompression can reduce headaches while relieving neck pain. Additionally, we communicate with certified medical providers who incorporate our patients’ information to reduce cervical spinal pain associated with headaches, causing many musculoskeletal issues in the upper body portion. We also inform them that non-surgical treatments can help relieve headaches and provide relief to the neck region. We encourage our patients to ask amazing educational questions for our associated medical providers about their symptoms correlating with cervical spinal pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer
Cervical Spinal Pain & Headache Connection
Throughout the world, neck pain (cervical spinal pain) is the second most common problem that can affect many individuals throughout their lives. It can lead to a life of disability and pain if not treated immediately. Many individuals often experience non-specific neck pain, as it can be through a postural or mechanical basis that can cause muscle strain in the surrounding muscles or compress the spinal canal to cause headaches that can last throughout the entire day. (Binder, 2008) Additionally, neck pain, like back pain, is a multifactorial disease with common risk factors like lack of physical activity, duration of computer usage, and perceived stress. (Kazeminasab et al., 2022) Many of these risk factors are normal as they can also affect the surrounding muscles in the lower back region and shoulder region, as many people often do repetitive motions that can naturally be overstretched and cause pain-like issues to the neck region. With neck pain connected with headaches, it can cause overlapping risk profiles and be costly. Neck pain associated with headaches can be a frequent and expensive occupational health problem as symptoms of pain, disability, reduced life quality, and, for adults, time lost for work. (Ben Ayed et al., 2019)
The correlation between headaches and neck pain is that the spinal canal is compressed from traumatic forces that can lead to cervicogenic headaches. Cervicogenic headaches usually aggravate neck mobility, thus reducing the ROM of the neck. (Verma, Tripathi, & Chandra, 2021) This can lead to many individuals suffering from migraine-like headaches and muscle stiffness in the upper regions of the body. When many individuals are dealing with headaches associated with cervical spinal pain, many will find treatments to mitigate the pain-like symptoms affecting the upper body region.
The Benefits Of Stretching-Video
When it comes to neck pain, it can be either acute or chronic depending the factors that cause it or the severity of the pain. Many individuals sought treatment that can alleviate the pain in the upper regions that are non-surgical and beneficial to their health and well-being. Non-surgical treatments can help stretch the tight and short muscles in the neck region and can reduce headaches affecting the person. Additionally, having the neck muscles professionally stretched by a massage therapist can relieve the neck and reduce headaches. The video above explains the benefits of stretching and describes how many people don’t stretch their bodies often to prevent pain-like issues from reoccurring in the future.
Spinal Decompression For Cervical Pain
Non-surgical treatments are excellent when it comes to reducing neck pain. When relieving neck pain, healthcare professionals must use the best available evidence to enhance clinical decision-making and improve the quality of care for people with neck pain. (Misailidou et al., 2010) Spinal decompression can help many people with neck pain by reducing the issues through gentle spinal traction. What spinal decompression does for the cervical spine is that it can realign the disc that is aggravating the neck region and causing headaches by stretching the surrounding muscles. This causes muscle improvement for the neck as it can change the patient’s pain outcome. (Youssef et al., 2019) Additionally, spinal decompression is safe, cost-effective, and gentle on the spine as it can be combined with other therapies to mitigate any residual pain that can relieve the neck and back. (Flynn, 2020) Many people who incorporate spinal decompression as part of their routine can benefit from their outcome as they return to their routine.
References
Ben Ayed, H., Yaich, S., Trigui, M., Ben Hmida, M., Ben Jemaa, M., Ammar, A., Jedidi, J., Karray, R., Feki, H., Mejdoub, Y., Kassis, M., & Damak, J. (2019). Prevalence, Risk Factors and Outcomes of Neck, Shoulders and Low-Back Pain in Secondary-School Children. J Res Health Sci, 19(1), e00440. www.ncbi.nlm.nih.gov/pubmed/31133629
Flynn, D. M. (2020). Chronic Musculoskeletal Pain: Nonpharmacologic, Noninvasive Treatments. American Family Physician, 102(8), 465-477. www.ncbi.nlm.nih.gov/pubmed/33064421
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. doi.org/10.1186/s12891-021-04957-4
Misailidou, V., Malliou, P., Beneka, A., Karagiannidis, A., & Godolias, G. (2010). Assessment of patients with neck pain: a review of definitions, selection criteria, and measurement tools. J Chiropr Med, 9(2), 49-59. doi.org/10.1016/j.jcm.2010.03.002
Verma, S., Tripathi, M., & Chandra, P. S. (2021). Cervicogenic Headache: Current Perspectives. Neurol India, 69(Supplement), S194-S198. doi.org/10.4103/0028-3886.315992
Youssef, J. A., Heiner, A. D., Montgomery, J. R., Tender, G. C., Lorio, M. P., Morreale, J. M., & Phillips, F. M. (2019). Outcomes of posterior cervical fusion and decompression: a systematic review and meta-analysis. Spine J, 19(10), 1714-1729. doi.org/10.1016/j.spinee.2019.04.019
Electromagnetic therapy of the knee joints, physiotherapist doctor uses medical equipment for highly effective pain treatment and inflammation, the magnetic field, rehabilitation.
The Q or quadriceps angle is a measurement of pelvic width that is believed to contribute to the risk of sports injuries in women athletes. Can non-surgical therapies and exercises help rehabilitate injuries?
Table of Contents
Quadriceps Q – Angle Injuries
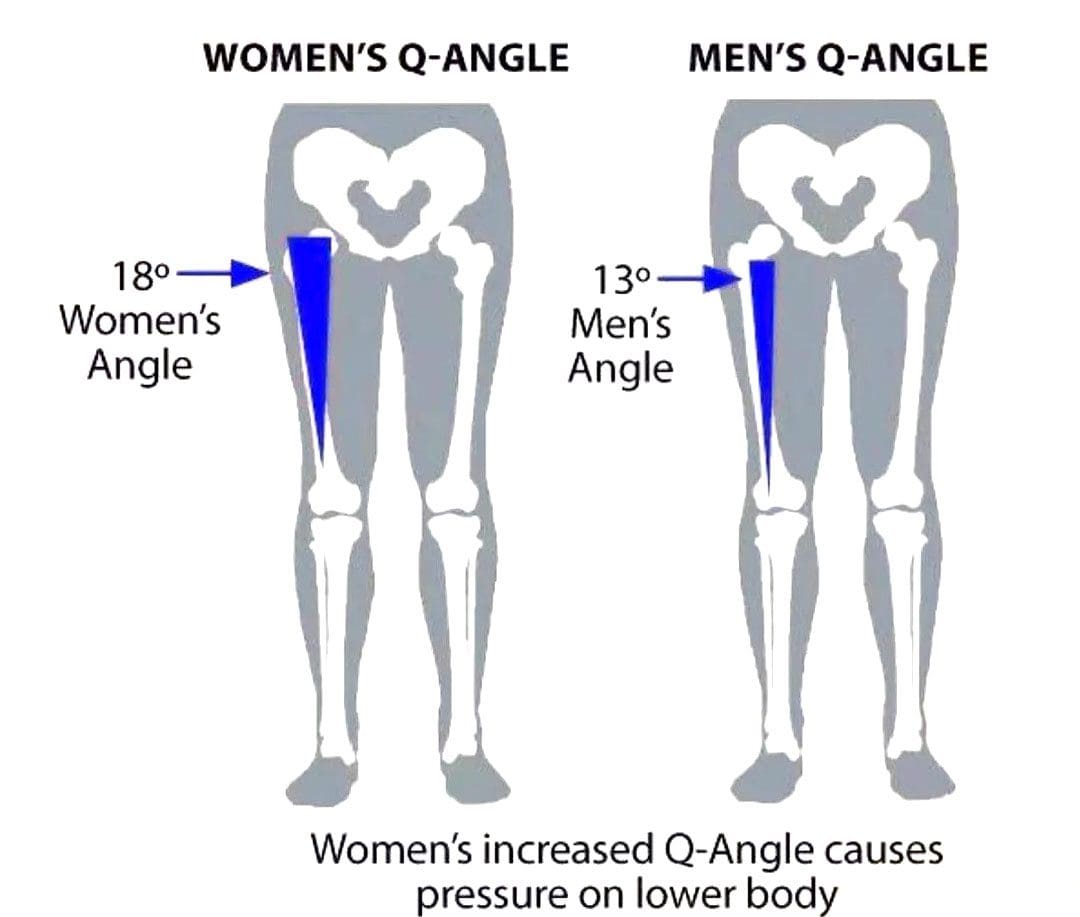
The Q angle is the angle where the femur/upper leg bone meets the tibia/lower leg bone. It is measured by two intersecting lines:
One from the center of the patella/kneecap to the anterior superior iliac spine of the pelvis.
The other is from the patella to the tibial tubercle.
On average the angle is three degrees higher in women than men.
Women have biomechanical differences that include a wider pelvis, making it easier to give birth. However, this difference can contribute to knee injuries when playing sports, as an increased Q angle generates more stress on the knee joint, as well as leading to increased foot pronation.
Injuries
Various factors can increase the risk of injury, but a wider Q angle has been linked to the following conditions.
Patellofemoral Pain Syndrome
An increased Q angle can cause the quadriceps to pull on the kneecap, shifting it out of place and causing dysfunctional patellar tracking.
With time, this can cause knee pain (under and around the kneecap), and muscle imbalance.
Foot orthotics and arch supports could be recommended.
Some researchers have found a link, while others have not found the same association. (Wolf Petersen, et al., 2014)
Chondromalacia of the Knee
This is the wearing down of the cartilage on the underside of the kneecap.
An increased Q angle can be a factor that increases stress and causes the knee to lose its stability.
However, this remains controversial, as some studies have found no association between the Q angle and knee injuries.
Chiropractic Treatment
Strengthening Exercises
ACL injury prevention programs designed for women have resulted in reduced injuries. (Trent Nessler, et al., 2017)
The vastus medialis obliquus or VMO is a teardrop-shaped muscle that helps move the knee joint and stabilize the kneecap.
Strengthening the muscle can increase the stability of the knee joint.
Strengthening may require a specific focus on muscle contraction timing.
Closed-chain exercises like wall squats are recommended.
Glute strengthening will improve stability.
Stretching Exercises
Stretching tight muscles will help relax the injured area, increase circulation, and restore range of motion and function.
Muscles commonly found to be tight include the quadriceps, hamstrings, iliotibial band, and gastrocnemius.
Foot Orthotics
Custom-made, flexible orthotics decrease the Q angle and reduce pronation, relieving the added stress on the knee.
A custom orthotic ensures that the foot and leg dynamics are accounted for and corrected.
Motion-control shoes can also help correct overpronation.
Knee Rehabilitation
References
Khasawneh, R. R., Allouh, M. Z., & Abu-El-Rub, E. (2019). Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one, 14(6), e0218387. doi.org/10.1371/journal.pone.0218387
Petersen, W., Ellermann, A., Gösele-Koppenburg, A., Best, R., Rembitzki, I. V., Brüggemann, G. P., & Liebau, C. (2014). Patellofemoral pain syndrome. Knee surgery, sports traumatology, arthroscopy: Official journal of the ESSKA, 22(10), 2264–2274. doi.org/10.1007/s00167-013-2759-6
Vaienti, E., Scita, G., Ceccarelli, F., & Pogliacomi, F. (2017). Understanding the human knee and its relationship to total knee replacement. Acta bio-medica : Atenei Parmensis, 88(2S), 6–16. doi.org/10.23750/abm.v88i2-S.6507
Mitani Y. (2017). Gender-related differences in lower limb alignment, range of joint motion, and the incidence of sports injuries in Japanese university athletes. Journal of Physical Therapy Science, 29(1), 12–15. doi.org/10.1589/jpts.29.12
Nessler, T., Denney, L., & Sampley, J. (2017). ACL Injury Prevention: What Does Research Tell Us? Current reviews in musculoskeletal medicine, 10(3), 281–288. doi.org/10.1007/s12178-017-9416-5
Sensitive Teeth. Young arab woman drinking water with ice and touching her cheek, sick middle eastern female frowning and rubbing inflamed area, suffering dental pain, emotionally reacting to cold
Temporomandibular joint disorder causes pain and jaw locking that can be worsened with certain activities. How individuals can manage and prevent flare-ups by learning what not to do to worsen the condition?
Table of Contents
What Not To Do Temporomandibular Joint Disorder
Tenderness, aching, pain, and jaw locking are symptoms of temporomandibular joint disorder or TMJ. The temporomandibular joint connects the jaw to the skull. It is used daily for eating, drinking, and talking. It is a small disc in the joint that allows the jaw bones to slip and slide correctly. With TMJ, the disc shifts out of place, leading to clicking, snapping, and limited jaw movement. It can also cause pain in the jaw and face, neck pain, and headaches, and the muscles around the jaw and neck can become sore and/or go into spasm. Any type of activity that stresses or overworks the joint can trigger a flare-up and worsen TMJ symptoms. (Schiffman E, et al. 2014) This article looks at avoiding activities that make TMJ worse and what not to do to help keep TMJ symptoms in check.
Chewing Gum
Gum chewing is not recommended for individuals with TMJ.
The jaw is one of the most used joints in the body.
Limiting excessive use alleviates pressure allowing the joints and muscles to rest.
Resting sore muscles and joints is the first step in injury recovery.
Eating Chewy and Hard Foods
Chewy and hard foods make the jaw have to work overtime.
Avoid eating hard foods like chewy candies, hard and chewy breads, and vegetables like corn on the cob, and fruits like apples.
These foods can place excessive stress on the jaw, and prevent the joint from properly resting and healing.
Chewing Only On One Side
Many individuals chew their food on only one side of the mouth.
This can stress out one side of the temporomandibular joint and surrounding muscles, leading to pain and dysfunction. (Urbano Santana-Mora, et al., 2013)
Stay aware of chewing habits and make sure to utilize both sides of the mouth.
Individuals with dental issues or tooth pain are recommended to see a dentist.
Non-Functional Jaw Activities
Going through each day, individuals tend to do things unconsciously or out of habit.
For example, individuals:
Reading or writing might chew on a pen or pencil.
Bite their nails or chew on the inside of their mouth while watching TV or internet browsing.
These activities can place stress on the joint, worsen the condition, and extend the healing process.
Resting on The Chin
Individuals will rest their jaw in their hands while studying, on social media, or watching TV.
This position can be comfortable, but it can affect the jaw.
This position can build pressure against the side of the jaw and push against the joint, causing the disc to shift out of place affecting how the jaw opens and closes.
Breaking the chin resting habit can allow the joint to relax and heal correctly.
Teeth Clenching
Bruxism is the medical term for clenching the teeth.
This can occur during the day or during sleep.
Teeth clenching is often brought on by stress and can place incredible pressure on the jaw’s muscles and worsen TMJ.
A dentist can prescribe a mouth guard to be worn while sleeping to protect the teeth from excessive clenching. (Miriam Garrigós-Pedrón, et al., 2019)
Slouching
The function of the jaw is closely related to body posture.
The jaw operates optimally when the head is above the cervical spine and the posture is upright.
Slouching can change how the jaw muscles work and the way the jaw opens and closes.
Part of physical therapy for TMJ is working on posture adjustments and training.
This can involve strengthening the back and shoulder muscles and setting up posture reminders.
Sitting and standing correctly can keep the jaw operating properly.
Postponing Treatment
Many with musculoskeletal issues and symptoms wait for the pain to go away.
Individuals having problems with their jaw should not wait to get treatment.
TMJ has a positive rate of recovery with conservative treatment, which is all the more reason to seek treatment. (G Dimitroulis. 2018)
A dentist or healthcare provider can provide an accurate diagnosis if TMJ is suspected.
Individuals can benefit from visiting a physical therapist to learn exercises and strategies to self-treat the condition. (Yasser Khaled, et al., 2017)
Treatment
Treatment can involve:
Initial treatment focuses on pain relief and jaw function opens and closes improvement.
A guard can help with night teeth grinding/bruxism.
Anti-inflammatory treatments.
In severe cases, surgery may be recommended to correct the problem, as a last resort. (Meghan K Murphy, et al., 2013)
Follow recommendations on what not to do and avoid certain activities.
Quick Patient Initiation
References
Schiffman, E., Ohrbach, R., Truelove, E., Look, J., Anderson, G., Goulet, J. P., List, T., Svensson, P., Gonzalez, Y., Lobbezoo, F., Michelotti, A., Brooks, S. L., Ceusters, W., Drangsholt, M., Ettlin, D., Gaul, C., Goldberg, L. J., Haythornthwaite, J. A., Hollender, L., Jensen, R., … Orofacial Pain Special Interest Group, International Association for the Study of Pain (2014). Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. Journal of oral & facial pain and headache, 28(1), 6–27. doi.org/10.11607/jop.1151
Santana-Mora, U., López-Cedrún, J., Mora, M. J., Otero, X. L., & Santana-Penín, U. (2013). Temporomandibular disorders: the habitual chewing side syndrome. PloS one, 8(4), e59980. doi.org/10.1371/journal.pone.0059980
Garrigós-Pedrón, M., Elizagaray-García, I., Domínguez-Gordillo, A. A., Del-Castillo-Pardo-de-Vera, J. L., & Gil-Martínez, A. (2019). Temporomandibular disorders: improving outcomes using a multidisciplinary approach. Journal of multidisciplinary healthcare, 12, 733–747. doi.org/10.2147/JMDH.S178507
Dimitroulis G. (2018). Management of temporomandibular joint disorders: A surgeon’s perspective. Australian Dental Journal, 63 Suppl 1, S79–S90. doi.org/10.1111/adj.12593
Khaled Y, Quach JK, Brennan MT, NapeÑas JJ. Outcomes after physical therapy for the treatment of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol, 2017;124(3: e190. doi:10.1016/j.oooo.2017.05.477
Abouelhuda, A. M., Khalifa, A. K., Kim, Y. K., & Hegazy, S. A. (2018). Non-invasive different modalities of treatment for temporomandibular disorders: a review of the literature. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 44(2), 43–51. doi.org/10.5125/jkaoms.2018.44.2.43
Murphy, M. K., MacBarb, R. F., Wong, M. E., & Athanasiou, K. A. (2013). Temporomandibular disorders: a review of etiology, clinical management, and tissue engineering strategies. The International journal of oral & maxillofacial implants, 28(6), e393–e414. doi.org/10.11607/jomi.te20
In individuals with herniated discs, how does non-surgical decompression compare to traditional surgery repair the spine?
Table of Contents
Introduction
When many individuals begin to add unnecessary pressure on their backs, it can lead to damaging results to their spine. The spine is the backbone of the body, allowing the upper and lower sections to be mobile and stabilizing the axial weight overload without the person feeling pain or discomfort. The spinal structure is surrounded by muscles, soft tissues, ligaments, nerve roots, and joints that support the spine. In between the spinal facet joints and structure are flat discs that absorb the shock and pressure from the axial overload. However, when unwanted stress starts to compress the disc, it can lead to the development of herniation. Depending on the location, it can cause pain-like symptoms like lower back and neck pain or sciatica. Other times, herniated discs can be due to natural degeneration, where the spinal disc height decreases, and it can crack under pressure, leading to disc dehydration, which, to this point, causes spinal issues to many individuals, thinking they are experiencing referred pain in different body locations. Coincidentally, many people can find the relief they seek through non-surgical treatments to restore the disc height and repair herniated discs. Today’s article focuses on the casing effects of herniated discs and how spinal decompression, a form of non-surgical treatment, can help reduce pain-like symptoms associated with herniated discs. Additionally, we communicate with certified medical providers who incorporate our patients’ information to reduce herniated disc pain, causing many musculoskeletal issues. We also inform them that non-surgical treatments can help mitigate the referred pain-like symptoms related to herniated discs and restore disc height in their spines. We encourage our patients to ask amazing educational questions for our associated medical providers about their referred pain correlating with herniated discs. Dr. Jimenez, D.C., incorporates this information as an educational service. Disclaimer
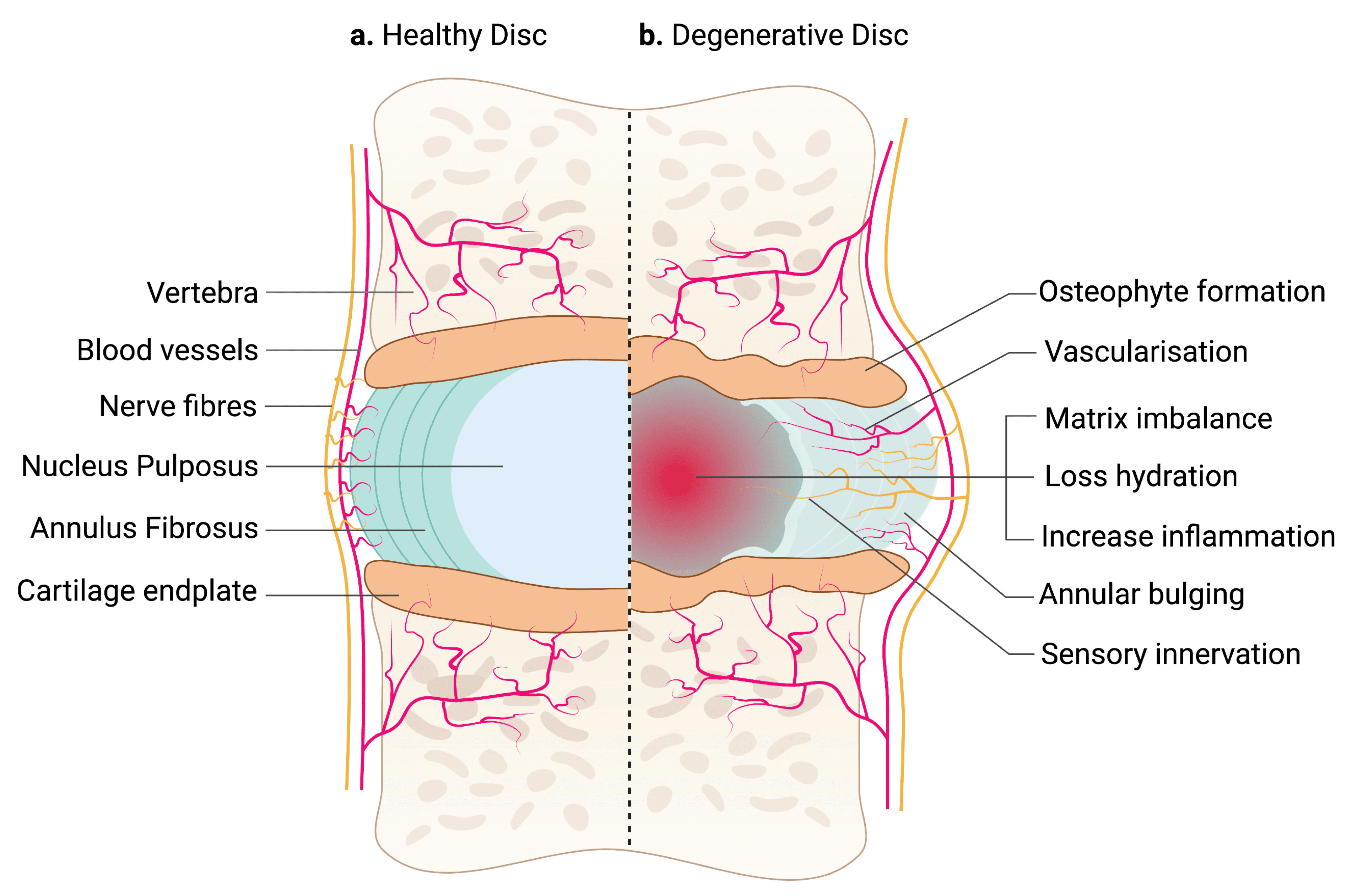
The Changing Effects Of Herniated Discs
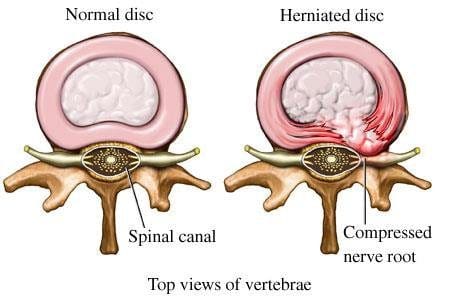
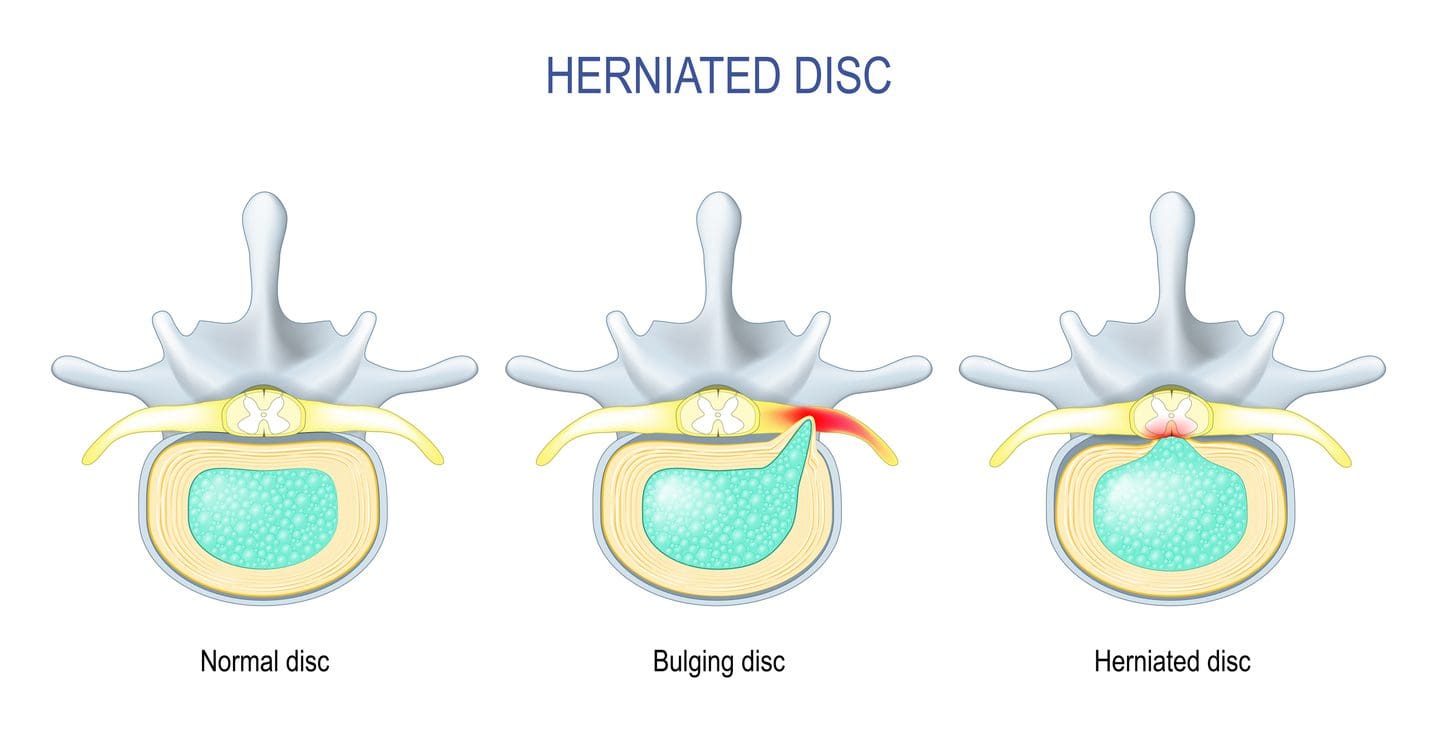
Have you experienced unwanted pain in your upper and lower extremities after a long work day? What about experiencing pain within your spines that are causing symptoms of numbness or tingling sensations in your hands, feet, or legs? Or are you dealing with excruciating lower back pain that is affecting your ability to work? Many individuals don’t realize that the pain-like symptoms they are experiencing are not low back, neck, or shoulder pain, but they correlate to herniated discs in their spines. Herniated discs are when the nucleus pulposus (inner disc portion) starts to protrude out of its original position from the intervertebral space. (Dydyk, Ngnitewe Massa, & Mesfin, 2023) Herniated discs are one of the common causes of lower back pain, and often, many individuals will remember what caused the herniation in their spine.
Some of the effects that lead to disc herniation are that many people will carry heavy objects constantly from one location to another, and the shifting weight can cause the disc to be continuously compressed and thus lead to herniation. Additionally, when the intervertebral disc starts showing signs of stiffness, it can result in abnormal spinal motion. (Haughton, Lim, & An, 1999) This causes morphologic changes within the intervertebral disc and causes it to be dehydrated. The chondroitin sulfation of the proteoglycan in the disc goes through changes in the disc itself, and when degeneration is associated with herniated discs, it can lead to musculoskeletal disorders. (Hutton et al., 1997)
The Root Cause Of Pain- Video
When degenerative changes start to affect the intervertebral discs, it can lead to intervertebral height loss, abnormal pain signaling, and nerve root entrapment associated with disc disruption. (Milette et al., 1999) This causes a cascading effect as the outer annulus of the spinal disc is cracked or ruptured, causing pain to the spine. When the outer annulus of the spinal disc starts to have nerve ingrowth in the affected discs, which then leads to individuals dealing with musculoskeletal disorders associated with pain. (Freemont et al., 1997) Many people will seek non-surgical therapies when finding treatment to alleviate the pain caused by herniated discs due to their cost-effectiveness and how it’s safe for their spine. Chiropractic care, massage therapy, spinal decompression, and traction therapy are available treatments that can be used in a personalized, inclusive treatment care plan to mitigate any pain the person is dealing with. The video explains how these treatments can use functional wellness principles to identify where the pain is located and treat any health issues with any potential underlying causes.
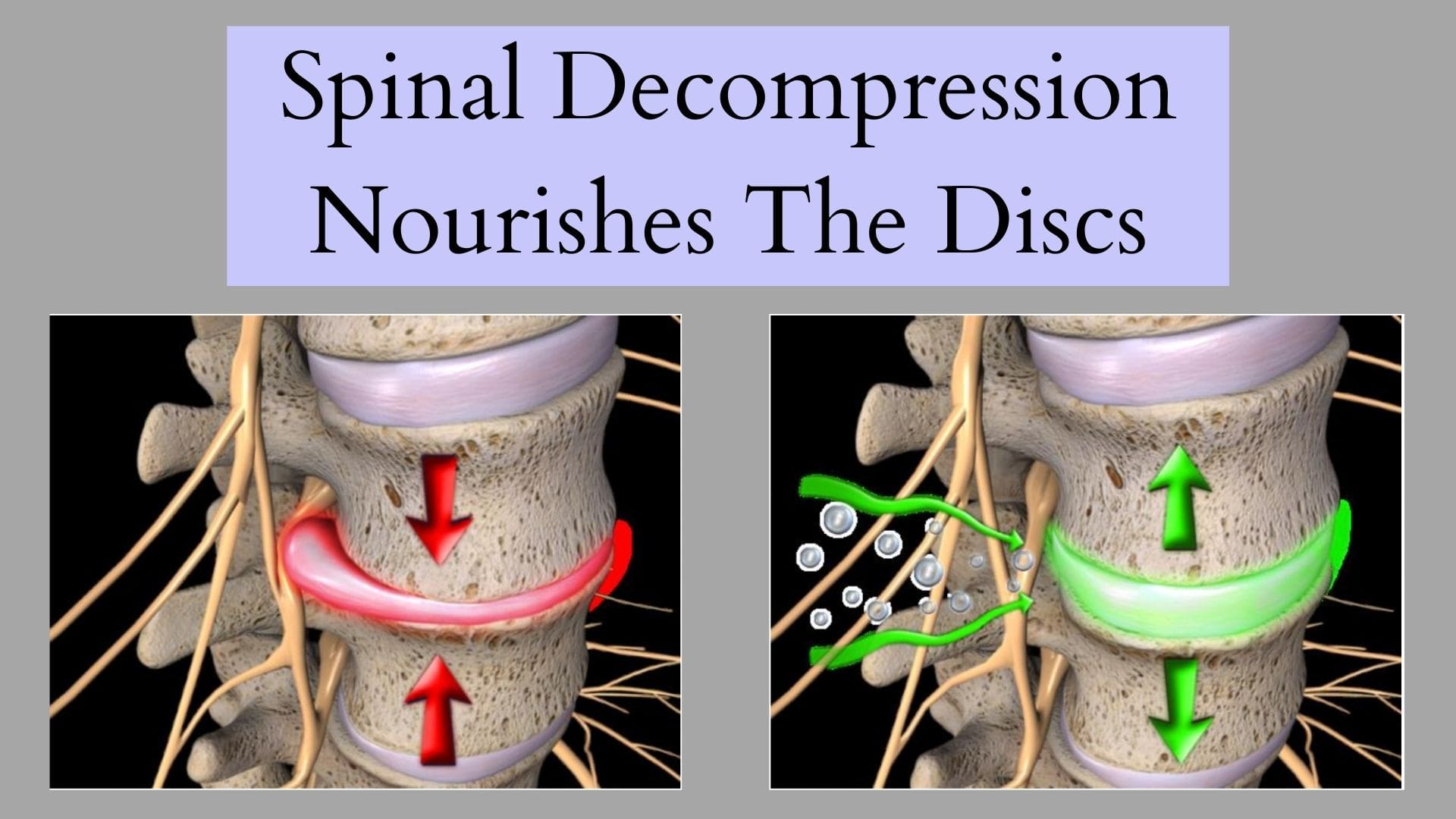
Spinal Decompression Reducing Herniated Disc
Regarding non-surgical treatments reducing herniated discs, spinal decompression can help mitigate the pain affecting the spine’s mobility. Spinal decompression utilizes mechanical traction to gently stretch the spine and allow the herniated disc to return to its original position. Spinal decompression incorporates negative pressure, which helps the nutrients increase the disc’s regenerative factors. (Choi et al., 2022) This allows the facet joints and aggravated nerves to have reduced pressure and increased disc space height. At the same time, spinal decompression can be combined with physical therapy to reduce the pain-like symptoms associated with herniated discs and provide beneficial results. (Amjad et al., 2022) Some of the beneficial factors related to spinal decompression include:
Pain improvement in the upper and lower extremities
Spinal range of motion
Muscle endurance restored
Joint ROM restored
When many individuals become more mindful of how different factors are causing spinal issues, they can make small routine changes in their daily lives, and that can reduce the chances of pain from returning. This allows them to enjoy life fully and continue their health and wellness journey.
References
Amjad, F., Mohseni-Bandpei, M. A., Gilani, S. A., Ahmad, A., & Hanif, A. (2022). Effects of non-surgical decompression therapy in addition to routine physical therapy on pain, range of motion, endurance, functional disability and quality of life versus routine physical therapy alone in patients with lumbar radiculopathy; a randomized controlled trial. BMC Musculoskelet Disord, 23(1), 255. doi.org/10.1186/s12891-022-05196-x
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P.-B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. doi.org/10.1155/2022/6343837
Freemont, A. J., Peacock, T. E., Goupille, P., Hoyland, J. A., O’Brien, J., & Jayson, M. I. (1997). Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet, 350(9072), 178-181. doi.org/10.1016/s0140-6736(97)02135-1
Haughton, V. M., Lim, T. H., & An, H. (1999). Intervertebral disk appearance correlated with stiffness of lumbar spinal motion segments. AJNR Am J Neuroradiol, 20(6), 1161-1165. www.ncbi.nlm.nih.gov/pubmed/10445464
Hutton, W. C., Elmer, W. A., Boden, S. D., Horton, W. C., & Carr, K. (1997). Analysis of chondroitin sulfate in lumbar intervertebral discs at two different stages of degeneration as assessed by discogram. Journal of Spinal Disorders, 10(1), 47-54. www.ncbi.nlm.nih.gov/pubmed/9041496
Milette, P. C., Fontaine, S., Lepanto, L., Cardinal, E., & Breton, G. (1999). Differentiating lumbar disc protrusions, disc bulges, and discs with normal contour but abnormal signal intensity. Magnetic resonance imaging with discographic correlations. Spine (Phila Pa 1976), 24(1), 44-53. doi.org/10.1097/00007632-199901010-00011
For individuals with pelvic pain, how does MET treatment strategies reduce muscle weakness in the hips region?
Table of Contents
Introduction
The pelvis’s main job is to ensure that the person’s body weight is distributed evenly for everyday movement within the upper and lower body. At the same time, the core muscles, ligaments, and joints surround the skeletal structure of the pelvis, which provides normal function while protecting the vital organ systems within the pelvic region. When normal or traumatic factors start to affect the body’s pelvic area, many individuals will often mistake the pain for low back pain, and the core muscles surrounding the pelvic bone can become weak and lead to pelvic pain. At the same time, normal factors like improper posture can cause anterior pelvic tilt and develop into other musculoskeletal disorders with overlapping risk profiles. When pelvic pain affects the lower extremities, it can also lead to reproductive issues that can cause even more stress to the individual. Luckily, many people opt for non-surgical treatments to reduce pelvic pain and its associated musculoskeletal condition by strengthening the weakened core muscles and reducing muscle weakness. Today’s article examines how referred pain symptoms affect the pelvis and how non-surgical treatments like MET therapy can reduce muscle weakness correlating with pelvic pain. Additionally, we communicate with certified medical providers who incorporate our patient’s information to reduce muscle weakness associated with pelvic pain. We also inform them that MET therapy can help mitigate the referred pain-like symptoms related to pelvic pain. We encourage our patients to ask amazing educational questions for our associated medical providers about their pelvic pain. Dr. Jimenez, D.C., incorporates this information as an educational service. Disclaimer
Referred Pain Symptoms Affecting The Pelvis
Have you noticed that you are taking more frequent trips to the bathroom and that your bladder still feels full? Do you experience muscle stiffness within your lower back or pelvic region from excessive sitting at your desk during work? Or do you notice that you are experiencing weak core muscles affecting your workout routine? These scenarios are associated with pelvic pain and can cause issues within the lower body extremities, affecting the person’s performance when doing normal activities. Pelvic pain is a multifactorial musculoskeletal disorder that can affect the corresponding body systems to induce referred pain. (Grinberg, Sela, & Nissanholtz-Gannot, 2020) Pelvic pain can cause referred pain to the gastrointestinal, pelvic musculoskeletal, and nervous systems, which then causes anatomic malfunction to the pelvic floor muscles. Pelvic pain can easily be mistaken for low back pain since the lumbar spine creates stressors for the muscles surrounding the pelvis.
When the pelvis is affected by mechanical stressors associated with the lumbar spine, it can cause pelvic dysfunction and causes the individual to be unbalanced when in motion. At the same time, the pelvic muscle structures will be overworked, leading to hip and joint destabilization, causing them to be weak. (Lee et al., 2016) When the pelvic muscle structures begin to destabilize, it can lead to sciatic nerve entrapment to the lower extremities, which leads to overlapping risk profiles for musculoskeletal disorders. When the surrounding pelvic muscles begin to entrap the pelvic nerve roots causing radiating pain down the legs. (Kale et al., 2021) However, there are ways to reduce referred pain affecting the pelvic region and restore muscle strength.
Sciatica, Causes, Symptoms, & Tips- Video
Since pelvic pain is a multifactorial musculoskeletal disorder that can lead to the development of referred pain to the lower body extremities, many individuals often think it is low back pain or sciatica. Referred pain is when pain affects a body location instead of where the source originated. Not treated immediately causes nerve entrapment, muscle weakness, and chronic pain within the reproductive and urinary organs. Many individuals seek non-surgical treatments to alleviate the pain and restore muscle strength to the body’s pelvic region. Non-surgical treatments like MET(muscle energy techniques) can help restore muscle strength to the pelvis through soft tissue stretching. Pain specialists specializing in MET therapy, like chiropractors and massage therapists, use hands-on maneuvers to relax, elongate, stretch, and massage the affected tight muscles and reduce any tender points that may have developed over time. (Grinberg et al., 2019) MET therapy can help stretch the pelvic stabilizing muscles. It can be combined with physical therapy and chiropractic care to realign the body and reduce nerve entrapment caused by pelvic pain. Check out the video above to learn more about the causes of sciatica and how non-surgical treatments may be the answer to alleviate pain.
MET Treatment Strategies For Pelvic Pain
MET therapy can reduce the effects of pelvic pain by including soft tissue manipulation methods to use controlled isometric and isotonic contraction to improve the normal physiologic function of the surrounding pelvic muscles and decrease pain and help stabilize the alternating structures within the pelvic region. (Sarkar, Goyal, & Samuel, 2021) MET therapy can also encourage self-regulating influences to reduce pain within the pelvic area, resulting in a greater range of motion. (Chaitow, 2009)
MET Treatment Reducing Muscle Weakness
MET therapy can also be part of a personalized health plan that can help restore muscle strength in the core and stabilize muscle within the pelvis. The positive effects of the combination of MET therapy and exercise, it can be more effective in reducing pain while improving physical function. (Hu et al., 2020) This allows the pelvis to realign itself and help stretch the shortened muscles. MET therapy can help restore low extremity function and improve a person’s quality of life. (Danazumi et al., 2021) MET therapy is an excellent way to stretch out tired muscles and restore pelvic function, as it can make individuals more mindful of their bodies while reducing the chances of pelvic pain associated with musculoskeletal disorders reoccurring again in the lower extremities.
Danazumi, M. S., Yakasai, A. M., Ibrahim, A. A., Shehu, U. T., & Ibrahim, S. U. (2021). Effect of integrated neuromuscular inhibition technique compared with positional release technique in the management of piriformis syndrome. J Osteopath Med, 121(8), 693-703. doi.org/10.1515/jom-2020-0327
Grinberg, K., Sela, Y., & Nissanholtz-Gannot, R. (2020). New Insights about Chronic Pelvic Pain Syndrome (CPPS). Int J Environ Res Public Health, 17(9). doi.org/10.3390/ijerph17093005
Grinberg, K., Weissman-Fogel, I., Lowenstein, L., Abramov, L., & Granot, M. (2019). How Does Myofascial Physical Therapy Attenuate Pain in Chronic Pelvic Pain Syndrome? Pain Res Manag, 2019, 6091257. doi.org/10.1155/2019/6091257
Hu, X., Ma, M., Zhao, X., Sun, W., Liu, Y., Zheng, Z., & Xu, L. (2020). Effects of exercise therapy for pregnancy-related low back pain and pelvic pain: A protocol for systematic review and meta-analysis. Medicine (Baltimore), 99(3), e17318. doi.org/10.1097/MD.0000000000017318
Kale, A., Basol, G., Topcu, A. C., Gundogdu, E. C., Usta, T., & Demirhan, R. (2021). Intrapelvic Nerve Entrapment Syndrome Caused by a Variation of the Intrapelvic Piriformis Muscle and Abnormal Varicose Vessels: A Case Report. Int Neurourol J, 25(2), 177-180. doi.org/10.5213/inj.2040232.116
Lee, D. W., Lim, C. H., Han, J. Y., & Kim, W. M. (2016). Chronic pelvic pain arising from dysfunctional stabilizing muscles of the hip joint and pelvis. The Korean Journal of Pain, 29(4), 274-276. doi.org/10.3344/kjp.2016.29.4.274
Sarkar, M., Goyal, M., & Samuel, A. J. (2021). Comparing the Effectiveness of the Muscle Energy Technique and Kinesiotaping in Mechanical Sacroiliac Joint Dysfunction: A Non-blinded, Two-Group, Pretest-Posttest Randomized Clinical Trial Protocol. Asian Spine Journal, 15(1), 54-63. doi.org/10.31616/asj.2019.0300
Should individuals with existing gastrointestinal problems eat bananas?
Table of Contents
Bananas
Bananas can be easy to digest and are often recommended for nausea and diarrhea, however, not everyone can tolerate them. (MedlinePlus. 2021)
Bananas are high in fructose, sorbitol, and soluble fiber, which makes them a common trigger for gastrointestinal problems.
Additionally, individuals not used to eating a high-fiber diet may find it helpful to gradually increase fiber and drink more water to alleviate unpleasant symptoms.
If there is a suspicion of intolerance, IBS, or malabsorption, it is recommended to speak with a healthcare provider for an evaluation.
Bananas can make the stomach hurt due to:
Irritable bowel syndrome (IBS)
Cramping
Gas
Bloating
Other gastrointestinal (GI) problems.
Individuals can experience stomach discomfort if there is a fructose intolerance or a rare banana allergy.
Stomach Pain
Bananas are used to replenish potassium and other essential nutrients lost from vomiting or diarrhea.
Some individuals can experience bloating and gas after eating them.
One reason is because of their soluble fiber content.
Soluble fiber dissolves in water and is more readily fermented in the colon than insoluble fiber.
Bananas also contain sorbitol – a naturally occurring sugar that acts as a laxative and can cause gas, bloating, and diarrhea when consumed in large amounts. (U.S. Food and Drug Administration. 2023)
Irritable Bowel Syndrome – IBS
Bananas can be a common trigger food for individuals with IBS.
Bananas are also high in fructose/simple sugar especially when they have overripened.
Individuals who have IBS are advised to avoid bananas because they can trigger many of the same side effects as undigested lactose/sugar in milk. (Johns Hopkins Medicine. 2023)
Ripe bananas are considered to be high in FODMAPS – fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.
Individuals following a low FODMAP diet to manage IBS may want to avoid or limit consumption.
Fructose malabsorption is when the body cannot digest or absorb fructose correctly. This causes bloating gas and abdominal discomfort.
Hereditary fructose intolerance is very rare. It happens when the liver cannot assist in the breakdown of fructose.
This condition often causes more severe symptoms and requires additional treatment besides removing fructose from an individual’s diet. (UW School of Medicine and Public Health. 2019)
Most can tolerate small amounts of fructose found in fruits like bananas.
If you’re eating bananas that are too green or unripe, you may also experience stomach discomfort.
Unripened bananas contain high amounts of resistant starch. In large quantities, this can cause mild symptoms like gas and bloating. (Jennifer M Erickson, et al., 2018)
Jackson Siegelbaum Gastroenterology. Colon gas and flatus prevention.
U.S. Food and Drug Administration. Sorbitol.
Capili, B., Anastasi, J. K., & Chang, M. (2016). Addressing the Role of Food in Irritable Bowel Syndrome Symptom Management. The journal for nurse practitioners: JNP, 12(5), 324–329. doi.org/10.1016/j.nurpra.2015.12.007
Johns Hopkins Medicine. 5 foods to avoid if you have IBS.
Monash University. Bananas re-tested.
Dayıoğlu A, Akgiray S, Nacaroğlu HT, Bahçeci Erdem S. The clinical spectrum of reactions due to banana allergy. BMB. 2020;5(2):60-63. doi: 10.4274/BMB.galenos.2020.04.013
Family Medicine Austin. Banana allergy.
UW School of Medicine and Public Health. Fructose-restricted diet.
Erickson, J. M., Carlson, J. L., Stewart, M. L., & Slavin, J. L. (2018). The Fermentability of Novel Type-4 Resistant Starches in In Vitro System. Foods (Basel, Switzerland), 7(2), 18. doi.org/10.3390/foods7020018
The Johns Hopkins Guide to Diabetes. What is resistant starch?
In individuals with discogenic low back pain, how does incorporating decompression reduce muscle strain in the back?
Table of Contents
Introduction
When it comes to low back pain, many people often complain that the surrounding muscles will ache constantly, and there is no relief from their primary doctors. Muscle strain associated with low back pain is one of the pain-like symptoms that many individuals experience when normal or traumatic factors start to cause issues in the lower back region of the body. When people begin to make constant repetitive motions correlating with normal daily activities like heavy lifting objects, poor posture, or stepping wrong, it can cause micro-tears to the surrounding muscles and the spinal discs in the lumbar region. When the spinal discs degenerate over time and have been under constant pressure, it can aggravate the surrounding nerve roots causing pain-like problems to the surrounding muscles, ligaments, and tissues, leading to musculoskeletal disorders corresponding with discogenic low back pain. Pain affecting the lower back can lead to a life of disability and make a person feel miserable. To that point, many individuals will seek non-surgical treatment to reduce discogenic pain associated with the low back and can find the relief they have sought. Today’s article examines how discogenic low back pain causes low back pain and how non-surgical treatments like decompression reduce discogenic low back pain and restore muscle strength. Additionally, we communicate with certified medical providers who incorporate our patient’s information to reduce muscle strain correlating with discogenic low back pain. We also inform them that decompression can help mitigate the pain-like symptoms associated with degenerated discs affecting the lower back region. We encourage our patients to ask amazing questions while looking for education from our associated medical providers about their low back issues. Dr. Jimenez, D.C., incorporates this information as an educational service. Disclaimer
Discogenic Low Back Pain Causing Muscle Strain
Do you often experience a pinched nerve or muscle strain in your lower back that hurts when standing? Do you feel symptoms of muscle spasms in your lower back or behind your legs? Or do you and your loved ones feel numbness or tingling sensations in your back, legs, and feet after sitting down excessively? These pain-like issues are associated with discogenic low back pain, which can lead to the development of disability in many people. Discogenic low back pain is developed when the intervertebral (spinal) disc degenerates over time and can contribute to disability. (Mohd Isa et al., 2022) When there are structural changes to the spinal disc that causes the degeneration to progress, it can lead to dysfunction and instability in the lumbar spine. The spinal discs in the spine have the primary job of absorbing the unwanted pressure load that the body is experiencing. Over time though, the spinal disc can degenerate and crack under pressure, leading to discogenic low back pain. Discogenic low back pain can lead to increased pain in the lower back region’s paraspinal muscles and muscle atrophy, inflammation, and muscle strain in the lower back muscles and lumbar spinal discs. (Huang et al., 2022) When the spinal disc is under constant pressure, the inflammatory cytokines can induce nerve ingrowth, structural and biomechanical changes, and a release of pain factors to contribute to the effects of discogenic low back pain. (Lyu et al., 2021) When people are dealing with discogenic low back pain associated with muscle strain, it can make them miss out on their daily activities.
From Injury To Recovery With Chiropractic-Video
When many individuals are experiencing discogenic low back pain, it can be difficult for pain specialists and doctors to identify the underlying source of pain since it is a multifactorial musculoskeletal disorder. (Fujii et al., 2019) However, numerous ways exist to reduce the pain and allow the individual to return to their daily routines. Non-surgical treatments are an excellent way to minimize the pain-like symptoms associated with discogenic low back pain. Treatments like decompression therapy and chiropractic care can create a happy experience for many individuals dealing with discogenic low back pain as it is safe, cost-effective, and gentle on the spine. Decompression can help reduce the pain in the posterior segment of the lumbar spine while relaxing the surrounding muscles and ligaments and pulling the affected disc back to its original position. (Choi et al., 2022) This creates negative pressure on the spinal column and increases disc height on the spine, which allows the fluids and nutrients to flood back into the spine and rehydrate the disc. Decompression therapy can also be combined with chiropractic care, as the spine can be manipulated mechanically or manually to allow the body to realign itself. This, in turn, promotes the body’s natural healing properties to work its magic and provide relief. The video explains how these treatments can positively impact many suffering individuals and help them regain their health.
Decompression Reducing Discogenic Low Back Pain
Decompression therapy allows the individuals to be strapped into a traction machine in a supine position and gently pulls the spine to enable the affected disc to return to the spine and lay off the pressure on the aggravating nerve root that is causing muscle strain. This causes the intervertebral disc space to change through negative pressure, which allows the height to increase in the intervertebral height without stimulating the surrounding fibers around the disc. (Oh et al., 2019) This allows the facet joints in the spine to be realigned, allowing them to be in their moveable location back to the spine to alleviate pain, thus restoring normal posture and activating body functions. When individuals incorporate decompression therapy consecutively, it can minimize the pain caused by discogenic low back pain and allows the individual to have a personalized plan to ensure the pain doesn’t return. (Macario et al., 2008)
Restoring Muscle Strength In The Low Back
Decompression therapy allows the affected muscle to be stretched gently, which can be strengthened through other treatments like physical therapy. This can effectively reduce discogenic low back pain associated with the affected discs and positively influence spinal mobility and muscle strength. (Wang et al., 2022) Even though degeneration in the spinal disc is a natural process, it is important to be mindful of the body to prevent pain-like symptoms from occurring and causing issues to the back. Decompression therapy can positively influence many individuals looking to regain their health and reduce the pain they are experiencing from discogenic low back pain so they can return to their daily activities.
References
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. doi.org/10.1155/2022/6343837
Fujii, K., Yamazaki, M., Kang, J. D., Risbud, M. V., Cho, S. K., Qureshi, S. A., Hecht, A. C., & Iatridis, J. C. (2019). Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment. JBMR Plus, 3(5), e10180. doi.org/10.1002/jbm4.10180
Huang, Y., Wang, L., Luo, B., Yang, K., Zeng, X., Chen, J., Zhang, Z., Li, Y., Cheng, X., & He, B. (2022). Associations of Lumber Disc Degeneration With Paraspinal Muscles Myosteatosis in Discogenic Low Back Pain. Front Endocrinol (Lausanne), 13, 891088. doi.org/10.3389/fendo.2022.891088
Lyu, F. J., Cui, H., Pan, H., Mc Cheung, K., Cao, X., Iatridis, J. C., & Zheng, Z. (2021). Painful intervertebral disc degeneration and inflammation: from laboratory evidence to clinical interventions. Bone Res, 9(1), 7. doi.org/10.1038/s41413-020-00125-x
Macario, A., Richmond, C., Auster, M., & Pergolizzi, J. V. (2008). Treatment of 94 outpatients with chronic discogenic low back pain with the DRX9000: a retrospective chart review. Pain Pract, 8(1), 11-17. doi.org/10.1111/j.1533-2500.2007.00167.x
Mohd Isa, I. L., Teoh, S. L., Mohd Nor, N. H., & Mokhtar, S. A. (2022). Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci, 24(1). doi.org/10.3390/ijms24010208
Oh, H., Choi, S., Lee, S., Choi, J., & Lee, K. (2019). Effects of the flexion-distraction technique and drop technique on straight leg raising angle and intervertebral disc height of patients with an intervertebral disc herniation. Journal of Physical Therapy Science, 31(8), 666-669. doi.org/10.1589/jpts.31.666
Wang, W., Long, F., Wu, X., Li, S., & Lin, J. (2022). Clinical Efficacy of Mechanical Traction as Physical Therapy for Lumbar Disc Herniation: A Meta-Analysis. Comput Math Methods Med, 2022, 5670303. doi.org/10.1155/2022/5670303
Can weight and strength training increase speed and power in athletes that participate in throwing sports?
Table of Contents
Throwing Sports
Top-throwing athletes have amazing arm speed. To succeed in throwing sports athletes need to be able to generate quick explosive power. This means the ability to propel the arm forward with substantial velocity for maximum object delivery like a baseball, javelin, hammer throw, shot put, discus, etc. Combined with sports technique training, throwing strength and power can be increased by training with weights. Here is a three-phase training plan to improve throwing performance.
Full Body
The arm provides only one part of the delivery process.
The legs, core, shoulders, and general flexibility need to work cooperatively to exert maximum thrust and achieve maximum object speed.
The natural ability to throw fast with power is largely determined by an individual’s muscle type, joint structure, and biomechanics. (Alexander E Weber, et al., 2014)
Preparation
Preparation should provide all-around muscle and strength conditioning for early pre-season conditioning.
Athletes will be doing throwing training as well, so fieldwork will need to be able to fit in.
It is recommended not to do weight training prior to throwing practice.
This leads to the start of competition and tournament play.
Frequency
2 to 3 sessions per week
Type
Strength and power – 60% to 70% for one-rep max/1RM
The one-repetition maximum test, known as a one-rep max or 1RM, is used to find out the heaviest weight you can lift once.
When designing a resistance training program, individuals use different percentages of their 1RM, depending on whether they’re lifting to improve muscular strength, endurance, hypertrophy, or power. (Dong-Il Seo, et al., 2012)
Throwing practice and competition are the priorities.
Before competition begins, take a 7- to 10-day break from heavyweight sessions while maintaining throwing workouts.
Weight training during competition should provide maintenance.
Frequency
1 to 2 sessions per week
Type
Power – lighter loads and faster execution than in the preparation stage.
Exercises
3 sets of 10
Rapid movement, 40% to 60% of 1RM.
Squats
Power hang clean and press
Romanian deadlift
Lat pulldown
Incline bench press
Crunches
Rest
Between sets 1 to 2 minutes.
Training Tips
Athletes have individual needs, so a general program like this needs modification based on age, sex, goals, skills, competitions, etc.
A certified strength and conditioning coach or trainer could help develop a fitness plan that can be adjusted as the athlete progresses.
Be sure to warm up prior to weight training and cool down afterward.
Don’t try to train through injuries or try to progress too fast – it is recommended not to throw or do weights when treating or recovering from an injury. (Terrance A Sgroi, John M Zajac. 2018)
Focus on the fundamentals and practice proper form.
Take a few weeks off at the end of the season to recover after hard training and competition.
Body Transformation
References
Weber, A. E., Kontaxis, A., O’Brien, S. J., & Bedi, A. (2014). The biomechanics of throwing: simplified and cogent. Sports medicine and arthroscopy review, 22(2), 72–79. doi.org/10.1097/JSA.0000000000000019
American College of Sports Medicine (2009). American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Medicine and science in sports and exercise, 41(3), 687–708. doi.org/10.1249/MSS.0b013e3181915670
Zaras, N., Spengos, K., Methenitis, S., Papadopoulos, C., Karampatsos, G., Georgiadis, G., Stasinaki, A., Manta, P., & Terzis, G. (2013). Effects of Strength vs. Ballistic-Power Training on Throwing Performance. Journal of sports science & medicine, 12(1), 130–137.
Seo, D. I., Kim, E., Fahs, C. A., Rossow, L., Young, K., Ferguson, S. L., Thiebaud, R., Sherk, V. D., Loenneke, J. P., Kim, D., Lee, M. K., Choi, K. H., Bemben, D. A., Bemben, M. G., & So, W. Y. (2012). Reliability of the one-repetition maximum test based on muscle group and gender. Journal of sports science & medicine, 11(2), 221–225.
Sakamoto, A., Kuroda, A., Sinclair, P. J., Naito, H., & Sakuma, K. (2018). The effectiveness of bench press training with or without throws on strength and shot put distance of competitive university athletes. European journal of applied physiology, 118(9), 1821–1830. doi.org/10.1007/s00421-018-3917-9
Sgroi, T. A., & Zajac, J. M. (2018). Return to Throwing after Shoulder or Elbow Injury. Current reviews in musculoskeletal medicine, 11(1), 12–18. doi.org/10.1007/s12178-018-9454-7
Wood block, transgender and sex equality backgrounds of male, female and lgbtq identity sign, choic.
Cisgender has nothing to do with an individual’s sexual orientation. Therefore how do sex and gender differ and where does cisgender fall within the spectrum of gender identities?
Table of Contents
Cisgender
Cisgender is a segment of the larger spectrum of gender identities. Also referred to as “cis,” it describes an individual whose gender identity corresponds to the sex they were assigned at birth. Therefore if an individual assigned sex at birth is female and identifies as a girl or a woman they are a cisgender woman.
The term describes how a person sees themselves and helps others communicate more accurately and respectfully.
Although many individuals may identify as cisgender, a cisgender person is not typical nor has qualities or characteristics that inherently differentiate them from a person of other gender identities.
Cisgender women commonly use the pronouns she and her.
A common mistake is using the term cis-gendered.
The proper usage of the term is cisgender.
Sex and Gender Differences
The terms sex and gender are often used interchangeably, however, they are not the same.
Sex is a biological and physiological designation based on an individual’s sex chromosomes and sexual organs.
This includes an individual’s genitals and sex organs.
It also encompasses secondary characteristics – like body size, bone structure, breast size, and facial hair – that are regarded as female or male.
Differences
Gender is a social construct that refers to roles and behaviors that society assigns as being masculine or feminine. The construct infers behaviors that are accepted or appropriate based on how an individual behaves, speaks, dresses, sits, etc.
Gender titles include sir, ma’am, mister, or miss.
Pronouns include him, she, he, and her.
Roles include actress, actor, prince, and princess.
Many of these suggest a power hierarchy of who has it and who does not.
Cisgender women often fall victim to these dynamics.
Sex
Refers to an individual’s chromosomes and the way that their genes are expressed.
Typically described in terms of male and female characteristics or the sex assigned at birth.
Gender
A social construct.
Refers to the social roles, behaviors, and expectations considered and/or deemed appropriate for men and women.
Historically defined as masculine and feminine, however, definitions can change as society changes.
Gender Identities Glossary
Today, gender is viewed as a spectrum where an individual might identify as one gender, more than one gender, or no gender. The definitions are often subtle and can often overlap, co-exist, and/or change. Gender identities include:
Cisgender
An individual whose gender identity matches their assigned sex at birth.
Transgender
An individual whose gender identity does not align with their assigned sex at birth.
Non-binary
An individual who feels their gender identity cannot be defined.
Demigender
An individual who experiences a partial, but not full/complete connection to a particular gender.
Agender
An individual who feels neither male nor female.
Genderqueer
Similar to non-binary but infers refusal of societal expectations.
Gender-neutral
Non-binary similarities but focuses on abandoning gender labels.
Gender fluid
An individual who experiences multiple genders or shifts between genders.
Polygender
An individual who experiences or expresses more than one gender.
Pangender
An individual who identifies with all genders.
Third gender
Third gender is a concept in which individuals are categorized, either by themselves or by society, as neither male nor female, not transitioning.
They are a different gender altogether.
Twin gender
A Native American term describing someone who is male and female or of two spirits simultaneously.
Cis Woman Identity
The terms cis woman or cis female are used to describe individuals who were assigned female at birth and identify as a woman or female. For cisgender woman, this means their gender identity aligns with their primary sex organs and secondary sex traits that include:
Higher pitch voice.
Wider pelvis.
Broadening of hips.
Breast development
It can also involve cisnormativity – a concept that everyone identifies as the gender they were assigned at birth. This could inform how a cis woman is expected to dress and act. An even more extreme concept is gender essentialism – this is the belief that gender differences are rooted purely in biology and cannot be changed. However, even cisnormativity beauty standards can influence the perceptions of transgender women that end up reinforcing gender stereotypes. (Monteiro D, Poulakis M. 2019)
Cisgender Privilege
Cisgender privilege is the concept that individuals who are cisgender receive added benefits compared to individuals who don’t conform to the gender binary norm. This includes cisgender women and men. Privilege happens when a cisgender individual assumes they are the norm and consciously or unconsciously takes action against those who are outside the definition of masculine and feminine. Examples of cisgender privilege include:
Not being denied work and social opportunities because of not fitting into the boy’s or girl’s club.
Not having to have sexual orientation questioned.
Not being denied healthcare due to provider discomfort.
Not fearing that civil rights or legal protections will be taken.
Not worrying about being bullied.
Not having to worry about attracting questioning looks in public.
Not being challenged or questioned about the clothes being worn.
Not being demeaned or mocked because of pronoun use.
Gender identity and sexual orientation are not the same.
A cisgender individual can be heterosexual, homosexual, bisexual, or asexual and so can a transgender individual.
Being cisgender has no correlation to an individual’s sexual orientation.
Chiropractic Care After Accidents and Injuries
References
Clayton, J. A., & Tannenbaum, C. (2016). Reporting Sex, Gender, or Both in Clinical Research? JAMA, 316(18), 1863–1864. doi.org/10.1001/jama.2016.16405
Monteiro, Delmira and Poulakis, Mixalis (2019) “Effects of Cisnormative Beauty Standards on Transgender Women’s Perceptions and Expressions of Beauty,” Midwest Social Sciences Journal: Vol. 22: Iss. 1, Article 10. DOI: doi.org/10.22543/2766-0796.1009 Available at: scholar.valpo.edu/mssj/vol22/iss1/10
Moleiro, C., & Pinto, N. (2015). Sexual orientation and gender identity: review of concepts, controversies and their relation to psychopathology classification systems. Frontiers in Psychology, 6, 1511. doi.org/10.3389/fpsyg.2015.01511
Can the effects of vertebral decompression relieve individuals with herniated discs and reduce intradiscal pressure on the spine?
Table of Contents
Introduction
The spine’s main job is to maintain the vertical pressure of the body without feeling pain or discomfort, especially when a person is in motion. The spinal discs are between the spinal joints, which are shock absorbers when pressure is implemented when a person is carrying a heavy object. The spinal column also has the spinal cord and nerve roots that are spread out from each section and have nerve root signals to be transmitted back and forth from the muscles to the brain to carry out its function. However, as the body ages, so does the spine, as many individuals are constantly adding unwanted pressure on their spines by doing normal factors and developing musculoskeletal disorders. At the same time, the spinal discs are also being affected as the unwanted pressure compresses them constantly, causing them to crack and herniate out of their position. To that point, the herniated disc aggravates the spinal nerve roots, leading to pain-like symptoms affecting the upper and lower body extremities. When this happens, many people will begin to experience musculoskeletal pain and cause overlapping risk profiles that cause their bodies to be misaligned. However, non-surgical treatments can be implemented as part of a daily routine for individuals dealing with herniated discs to reduce intradiscal pressure off the affected muscles in the upper and lower body extremities and restore functionality to the body. Today’s article focuses on why herniated disc affects many people and how vertebral traction can reduce intradiscal pressure off the spine while relieving the musculoskeletal system. Additionally, we work hand-in-hand with certified medical providers who incorporate our patient’s information to reduce intradiscal stress correlating with herniated discs. We also inform them that vertebral traction therapy (spinal decompression) can help mitigate the pain-like symptoms associated with herniated discs and provide relief to the body. We encourage our patients to ask profound questions while seeking education from our associated medical providers about their pain-like issues. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
Why Does Herniated Disc Affect People?
Have you or your loved ones been dealing with muscle aches or strains in their back, neck, or shoulders after carrying/lifting a heavy object? Do you feel a numbing or tingling sensation in your hands, legs, or feet after a long day after work? Or have you been constantly dealing with muscle and joint stiffness after a long workday? At some point in their lives, everyone has dealt with pain affecting their upper and lower extremities, leading to herniated discs in the spine’s upper, middle, or lower portions. As stated earlier, the body and the spine age naturally, leading to the development of herniated discs in the spine. Disc herniation occurs when the nucleus pulposus (inner disc layer) starts to break through the weaker annulus fibrosus (outer disc layer) and compress the surrounding nerve root, leading to an overlapping risk profile to the upper and lower body portions. (Ge et al., 2019) Disc herniation is developed when the spine goes through a natural degeneration, which causes them to be more susceptible to microtears. When individuals start to do normal activities like lifting or carrying heavy objects, it can enhance the progression further, leading to musculoskeletal disorders. Additionally, the spinal degeneration associated with disc herniation can cause inflammatory responses when the protruding disc is compressing the nerve roots, which then causes symptoms of pain and numbness to the upper and lower extremities. (Cunha et al., 2018)
Why do herniated discs cause inflammatory responses to the compressed nerve roots that cause pain-like symptoms to the upper and lower body extremities? Well, when many individuals are experiencing pain associated with herniated discs, they believe they are dealing with upper or lower pain, depending on where the herniated disc is located. This causes referred pain symptoms where the pain is being perceived in one location than the site where the pain is originating. Coincidentally, when individuals are doing repetitive motions associated with herniated discs can cause the adjacent nerve root to be compressed, which then causes the surrounding muscles, ligaments, and soft tissues to be in pain. (Blamoutier, 2019) Pain developing from herniated discs can reduce a person’s quality of life and make them miss out on important life events.
Disc Herniation Overview-Video
Many factors associated with a herniated disc can lead to its development and range from mild to severe depending on where the disc is herniated. Since the spine and spinal disc do degenerate over time naturally, it can cause the disc to crack and dehydrate. This leads to restricted movement, the development of neck, back, and shoulder pain, a decrease in muscle strength in the extremities, and numbness. (Jin et al., 2023) These are some results when herniated discs are not being treated right away. Luckily there are non-surgical treatments to alleviate the pain-like symptoms associated with herniated discs and help reduce intradiscal pressure in the spine while restoring spinal mobility and muscle strength. Spinal decompression, chiropractic care, massage therapy, and physical therapy are some non-surgical treatments that can help alleviate herniated discs and its associated symptoms. Non-surgical treatments can help pull the herniated disc off the compressed nerve root through manual and mechanical manipulation and return it to its original position. Additionally, non-surgical treatments can be part of a daily health and wellness routine combined with other therapies to reduce pain-like symptoms associated with herniated discs and help restore the spine’s mobility. The video above explains the causes, factors, and symptoms associated with herniated discs and how these treatments can alleviate the pain.
The Effects Of Vertebral Traction On Disc Herniation
Non-surgical treatments like vertebral decompression can provide a positive outlook when reducing the effects of herniated discs. Vertical or spinal decompression can help reduce the underlying problem associated with herniated discs by relieving the pain and intradiscal pressure off the vital structures of the spine. (Ramos & Martin, 1994) Additionally, vertebral decompression uses gentle traction to relieve nerve pain associated with herniated discs. It helps reduce the compression force on the affected spinal discs, reducing nerve compression by expanding the disc height in the spine. (Wang et al., 2022)
With spinal decompression being incorporated to reduce the effects of herniated discs, individuals are strapped into a traction machine in a supine position. They will feel a mechanical pull to their spines as the herniated disc returns to its original position and the height of the spinal disc increases. (Oh et al., 2019) This allows the negative pressure from the traction to increase the body’s blood flow for the nutrients and fluids to rehydrate the discs while allowing the body’s natural healing process to kick into full gear. (Choi et al., 2022) After a few consecutive sessions with spinal decompression, many individuals will notice that the pain in their neck, back, and shoulders has decreased and that they can return to their daily activities. Spinal decompression allows the individual to regain their health and well-being while also reminding them to be more mindful of what certain factors can cause the pain to return to the spine. By being more aware of what is affecting a person’s body, they have the tools to continue their health and wellness journey.
References
Blamoutier, A. (2019). Nerve root compression by lumbar disc herniation: A french discovery? Orthop Traumatol Surg Res, 105(2), 335-338. doi.org/10.1016/j.otsr.2018.10.025
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. doi.org/10.1155/2022/6343837
Cunha, C., Silva, A. J., Pereira, P., Vaz, R., Goncalves, R. M., & Barbosa, M. A. (2018). The inflammatory response in the regression of lumbar disc herniation. Arthritis Res Ther, 20(1), 251. doi.org/10.1186/s13075-018-1743-4
Ge, C. Y., Hao, D. J., Yan, L., Shan, L. Q., Zhao, Q. P., He, B. R., & Hui, H. (2019). Intradural Lumbar Disc Herniation: A Case Report and Literature Review. Clin Interv Aging, 14, 2295-2299. doi.org/10.2147/CIA.S228717
Jin, Y. Z., Zhao, B., Zhao, X. F., Lu, X. D., Fan, Z. F., Wang, C. J., Qi, D. T., Wang, X. N., Zhou, R. T., & Zhao, Y. B. (2023). Lumbar Intradural Disc Herniation Caused by Injury: A Case Report and Literature Review. Orthopaedic Surgery, 15(6), 1694-1701. doi.org/10.1111/os.13723
Oh, H., Choi, S., Lee, S., Choi, J., & Lee, K. (2019). Effects of the flexion-distraction technique and drop technique on straight leg raising angle and intervertebral disc height of patients with an intervertebral disc herniation. Journal of Physical Therapy Science, 31(8), 666-669. doi.org/10.1589/jpts.31.666
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. doi.org/10.3171/jns.1994.81.3.0350
Wang, W., Long, F., Wu, X., Li, S., & Lin, J. (2022). Clinical Efficacy of Mechanical Traction as Physical Therapy for Lumbar Disc Herniation: A Meta-Analysis. Comput Math Methods Med, 2022, 5670303. doi.org/10.1155/2022/5670303
Female doctor talking to patient points to vertebrae on spine model telling principle of treatment. Serious doctor talking to young woman sitting at table in medical office. Concept of vertebrology.
While a healthy, sustainable lifestyle for one individual may not be the best option for another, can experts point out signs of a healthy life?
Table of Contents
Healthy Life
Being or living a healthy life is a phrase that can be confusing. Researchers examine some major areas of concern with constant imagery like social media’s role in shaping what behaviors people consider important to reach a physical fitness/health goal. These behaviors prioritize physical appearance and are often linked with negative psychological effects and worsening physical health outcomes. (Binder A, et al., 2021) Studies routinely show that someone’s body shape is not a good indicator of how healthy they really are. (Uhlmann LR, et al., 2018)
Living a healthy life is a multi-faceted endeavor that requires maintaining a balance. New research has shown that “adhering to both quality diet and sufficient physical activity is important for optimally reducing the risk of mortality from all causes, CVD and PDAR cancers.” (Ding D, et al., 2022) Individuals do not need to make extreme changes to these areas of their lifestyle. Studies show that making small adjustments, little by little, prepares the individual to develop long-term sustainable habits. (Adhikari P, Gollub E. 2021)
Nutritional Health
Too much salt, sugar, and saturated fat increases the risk of diseases like diabetes, heart disease, and stroke. (National Institutes of Health, 2017) It can be easy to overlook balanced nutrition and it is not all about what should be restricted and avoided. It is about making sure the body gets the proper amount of nutrient-rich foods essential to overall health. Examples include:
Deficiency of nutrients like magnesium, calcium, and vitamins A, C, D, E, and K are with sleep problems. (Ikonte CJ, et al., 2019)
Not acquiring enough protein can lead to slowed metabolism and weight gain. (Pezeshki A, et al., 2016)
Healthy fats are essential to protect against heart disease and can help maintain high energy levels. (Gammone MA, et al., 2018)
Research has found that depression and nutrition are linked.
Incorporating a diet like the Mediterranean has been associated with a reduced risk of depression symptoms. (Oddo VM, et al., 2022)
Physical Activity
Regular physical activity helps with weight management, reduces the risk of chronic diseases, maintains healthy bones and joints, and contributes to positive mental health and mood.
The Centers for Disease Control and Prevention estimates around 60 percent of the population does not get enough daily physical activity. (Surgeon General Report, CDC. 1999)
According to the research, individuals don’t exercise for consistent reasons that include: not having enough time, no access to resources, and being too tired to work out. (Yen Sin Koh, et al., 2022)
Increasing the heart rate for only 12 minutes a day can protect the cardiovascular system. (Matthew Nayor, et al., 2020)
Signs
A few signs that an individual is healthy.
Stable Energy Levels
Having energy throughout the day is a sign you’re getting high-quality sleep.
Energy levels can also offer clues on nutritional intake, particularly of fats, carbohydrates, and proteins. (Yohannes Adama Melaku, et al., 2019)
The right combination of macronutrients can be different for everyone, especially depending on factors like age, job, medical history, and physical activity.
Paying attention to energy levels at different times of the day can help guide fitness and health goals.
One sign that the mind and body are dealing with stress well is the ability to set boundaries.
Setting boundaries shows recognition and priority for their needs.
This could be boundaries for respect of thoughts and ideas, physical space, emotional needs, the time spent on certain things, sex life, and material possessions.
Fresh Breath
The mouth can show what is going on as far as the health of the body.
Poor oral hygiene can lead to a buildup of bacteria that can spread throughout the respiratory and digestive tracts.
Chronic bad breath is a common sign of poor oral health.
Studies suggest that increased bacteria entering the body can lower immune system response and increase the development of general health problems. (NIH. 2018)
Time to Change
Signs that the mind and body are not healthy include:
Always sick or feel as if you’re coming down with something.
The stomach is constantly feeling like it is bloated, backed up, or dealing with acid reflux or indigestion.
The human body, organs, and tissues are complex structures, and the signals they transmit about underlying issues can be subtle which individuals tend to not notice until the little problems become major ones. It’s important to look at life habits and be honest about changes that may need to be implemented to improve health, lessen the risk of chronic health conditions, and improve quality of life.
Multidisciplinary Evaluations and Treatment
References
Binder, A., Noetzel, S., Spielvogel, I., & Matthes, J. (2021). “Context, Please?” The Effects of Appearance- and Health-Frames and Media Context on Body-Related Outcomes. Frontiers in public health, 9, 637354. doi.org/10.3389/fpubh.2021.637354
Uhlmann, L. R., Donovan, C. L., Zimmer-Gembeck, M. J., Bell, H. S., & Ramme, R. A. (2018). The fit beauty ideal: A healthy alternative to thinness or a wolf in sheep’s clothing? Body image, 25, 23–30. doi.org/10.1016/j.bodyim.2018.01.005
Ding, D., Van Buskirk, J., Nguyen, B., Stamatakis, E., Elbarbary, M., Veronese, N., Clare, P. J., Lee, I. M., Ekelund, U., & Fontana, L. (2022). Physical activity, diet quality and all-cause cardiovascular disease and cancer mortality: a prospective study of 346 627 UK Biobank participants. British Journal of sports medicine, bj sports-2021-105195. Advanced online publication. doi.org/10.1136/bjsports-2021-105195
Adhikari, P., & Gollub, E. (2021). Evaluation of the Small Changes, Healthy Habits Pilot Program: Its Influence on Healthy Eating and Physical Activity Behaviors of Adults in Louisiana. European journal of investigation in health, psychology, and education, 11(1), 251–262. doi.org/10.3390/ejihpe11010019
How dietary factors influence disease risk. National Institutes of Health (NIH)
Ikonte, C. J., Mun, J. G., Reider, C. A., Grant, R. W., & Mitmesser, S. H. (2019). Micronutrient Inadequacy in Short Sleep: Analysis of the NHANES 2005-2016. Nutrients, 11(10), 2335. doi.org/10.3390/nu11102335
Pezeshki, A., Zapata, R. C., Singh, A., Yee, N. J., & Chelikani, P. K. (2016). Low protein diets produce divergent effects on energy balance. Scientific reports, 6, 25145. doi.org/10.1038/srep25145
Gammone, M. A., Riccioni, G., Parrinello, G., & D’Orazio, N. (2018). Omega-3 Polyunsaturated Fatty Acids: Benefits and Endpoints in Sport. Nutrients, 11(1), 46. doi.org/10.3390/nu11010046
Oddo, V. M., Welke, L., McLeod, A., Pezley, L., Xia, Y., Maki, P., Koenig, M. D., Kominiarek, M. A., Langenecker, S., & Tussing-Humphreys, L. (2022). Adherence to a Mediterranean Diet Is Associated with Lower Depressive Symptoms among U.S. Adults. Nutrients, 14(2), 278. doi.org/10.3390/nu14020278
Adults, Surgeon General Report, CDC.
Koh, Y. S., Asharani, P. V., Devi, F., Roystonn, K., Wang, P., Vaingankar, J. A., Abdin, E., Sum, C. F., Lee, E. S., Müller-Riemenschneider, F., Chong, S. A., & Subramaniam, M. (2022). A cross-sectional study on the perceived barriers to physical activity and their associations with domain-specific physical activity and sedentary behavior. BMC public health, 22(1), 1051. doi.org/10.1186/s12889-022-13431-2
Saint-Maurice, P. F., Graubard, B. I., Troiano, R. P., Berrigan, D., Galuska, D. A., Fulton, J. E., & Matthews, C. E. (2022). Estimated Number of Deaths Prevented Through Increased Physical Activity Among US Adults. JAMA internal medicine, 182(3), 349–352. doi.org/10.1001/jamainternmed.2021.7755
Nayor, M., Shah, R. V., Miller, P. E., Blodgett, J. B., Tanguay, M., Pico, A. R., Murthy, V. L., Malhotra, R., Houstis, N. E., Deik, A., Pierce, K. A., Bullock, K., Dailey, L., Velagaleti, R. S., Moore, S. A., Ho, J. E., Baggish, A. L., Clish, C. B., Larson, M. G., Vasan, R. S., … Lewis, G. D. (2020). Metabolic Architecture of Acute Exercise Response in Middle-Aged Adults in the Community. Circulation, 142(20), 1905–1924. doi.org/10.1161/CIRCULATIONAHA.120.050281
Melaku, Y. A., Reynolds, A. C., Gill, T. K., Appleton, S., & Adams, R. (2019). Association between Macronutrient Intake and Excessive Daytime Sleepiness: An Iso-Caloric Substitution Analysis from the North West Adelaide Health Study. Nutrients, 11(10), 2374. doi.org/10.3390/nu11102374
Jamieson, J. P., Black, A. E., Pelaia, L. E., Gravelding, H., Gordils, J., & Reis, H. T. (2022). Reappraising stress arousal improves affective, neuroendocrine, and academic performance outcomes in community college classrooms. Journal of experimental psychology. General, 151(1), 197–212. doi.org/10.1037/xge0000893
Vernia, F., Di Ruscio, M., Ciccone, A., Viscido, A., Frieri, G., Stefanelli, G., & Latella, G. (2021). Sleep disorders related to nutrition and digestive diseases: a neglected clinical condition. International journal of medical sciences, 18(3), 593–603. doi.org/10.7150/ijms.45512
Can spinal decompression treatments be incorporated for individuals with lumbosacral pain and improve posture?
Table of Contents
Introduction
Many individuals only realize they have poor posture once they perform a movement that causes pain in the lumbosacral region of their body. Have you or your loved ones experienced muscle aches or strains after relaxing in a weird position? Or do you begin to notice that you are hunched over when walking from one location to another? Many of these scenarios correspond to how we present ourselves with our posture. Our posture helps support the upper body’s weight while stabilizing the lower body through the spine and ensuring that our body is in an upright position when we are in motion. However, as we age, so do our bodies and spine, which then causes us to be in a hunched position, causing our posture to degenerate. This causes lumbosacral pain to develop along the body’s lower extremities, leading to overlapping risk profiles that cause mobility issues, poor posture, and disability if not treated right away. When this happens, the surrounding muscles, ligaments, and tissues around the lumbar spine will begin to develop pain-like symptoms and can make a person’s life miserable. Luckily there are various techniques and treatments to improve poor posture and reduce lumbosacral pain affecting many individuals. Today’s article looks at how lumbosacral pain affects a person’s posture and how spinal decompression and MET therapy can reduce lumbosacral pain and restore good posture. Additionally, we work hand-in-hand with certified medical providers who incorporate our patient’s information to treat and minimize lumbosacral pain associated with poor posture. We also inform them that spinal decompression combined with MET therapy can help with lumbosacral pain while improving good posture back to the body. We encourage our patients to ask profound questions while seeking education from our associated medical providers about their pain-like issues. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
Lumbosacral Pain Affects Posture
Have you noticed you are constantly slouching or being in a hunched position, only to feel muscle aches and strains in your lumbar-sacral region? Do you feel symptoms of tingling and numbness in your hips and buttock region after sitting down excessively? Or do you feel referred pain in one location and have to shift your weight to compensate for the pain? These pain-like symptoms and scenarios correspond to lumbosacral pain affecting your posture. The lumbosacral spine region has a natural curve that functions as a shock absorber to mitigate the body’s mechanical weight and stress when in motion. (Adams & Hutton, 1985) At the same time, it is susceptible to being constantly injured as the spinal disc is being compressed and can be herniated or damaged over time, manifesting into lumbosacral pain. So how does lumbosacral pain associate with poor posture? When individuals are dealing with low back problems associated with lumbosacral pain, the spinal disc in the lumbosacral region starts to have balancing issues when in motion. (Huang, Jaw, & Young, 2022) When people are dealing with difficulties balancing their gait cycle, it can cause their walking performance and postural control to be dysfunctional and cause the body to be misaligned, thus causing musculoskeletal issues to arise and affecting the lower body and its extremities. The surrounding muscles surrounding the lumbosacral region will begin to experience stiffness in the trunk region, which can cause musculoskeletal changes to the surrounding muscles when individuals start to be in an upright position. (Creze et al., 2019) When poor posture affects the trunk muscles, the surrounding accessory muscles start acting to compensate for the pain. To that point, lumbosacral pain associated with poor posture could lead to abdominal, low back, hip, and pelvic pain. However, many individuals can find various therapies and relieving techniques to improve posture, strengthen the surrounding muscles, and reduce pain-like symptoms.
Building A Stronger Body- Video
Many individuals can seek out various non-invasive therapies to alleviate the issue when it comes to improving posture and reducing lumbosacral pain. These therapies are cost-effective and personalized to the person’s pain. Treatments like chiropractic care and decompression can help restore good posture while realigning the body out of subluxation and help stretch the affected muscles. Coincidentally, non-surgical therapies can be combined with other treatments like physical therapy to strengthen the trunk muscles surrounding the lumbosacral region, thus reducing the load on the lumbosacral spine. (Callaghan, Gunning, & McGill, 1998) When people focus on their health and well-being, non-surgical therapies can provide a positive and safe experience with a team that can help reduce the pain the person has been dealing with their entire lives. The video above explains how these treatments work together to help you build a stronger body while revitalizing your energy and enhancing your health and wellness.
Spinal Decompression Reducing Lumbosacral Pain
When it comes to reducing lumbosacral pain associated with poor posture, many individuals can incorporate non-surgical treatments like spinal decompression and combine them with a personalized treatment plan to reduce the pain-like symptoms. What spinal decompression does to lumbosacral pain is that it helps mitigate intra-disc pressure while increasing disc space within the lumbosacral spinal region. (Amjad et al., 2022) Spinal decompression can help improve leg mobility and stretch out the affected muscles to kick-start the body’s natural healing process. Spinal decompression can even combine with physical therapy to help strengthen the lumbosacral region’s abdominal muscles and enable many individuals with poor posture to be mindful of how they present themselves.(Mielenz et al., 1997)
MET Therapy & Spinal Decompression Restoring Posture
When pain specialists like chiropractors and massage therapists incorporate spinal decompression treatment to reduce lumbosacral pain, they also utilize various techniques to strengthen the lumbosacral muscles to restore proper posture to the body. Many pain specialists use MET (muscle energy techniques) therapy to maintain while stretching the muscles and fascia in the affected areas. MET therapy combined with spinal decompression can help improve muscle shortness in the lumbar fascial tissue, improve posture, and even increase the lumbar and pelvic range of motion. (Tamartash & Bahrpeyma, 2022) These two non-surgical treatments can help many people by addressing their posture and movement dysfunction while strengthening their core stabilized muscles to reduce pain. (Norris & Matthews, 2008) Many individuals who want to regain their health and wellness can make small changes in their routine to improve their posture and be more mindful of their bodies to reduce the chances of lumbosacral pain returning.
References
Adams, M. A., & Hutton, W. C. (1985). The effect of posture on the lumbar spine. J Bone Joint Surg Br, 67(4), 625-629. doi.org/10.1302/0301-620X.67B4.4030863
Amjad, F., Mohseni-Bandpei, M. A., Gilani, S. A., Ahmad, A., & Hanif, A. (2022). Effects of non-surgical decompression therapy in addition to routine physical therapy on pain, range of motion, endurance, functional disability and quality of life versus routine physical therapy alone in patients with lumbar radiculopathy; a randomized controlled trial. BMC Musculoskelet Disord, 23(1), 255. doi.org/10.1186/s12891-022-05196-x
Callaghan, J. P., Gunning, J. L., & McGill, S. M. (1998). The relationship between lumbar spine load and muscle activity during extensor exercises. Phys Ther, 78(1), 8-18. doi.org/10.1093/ptj/78.1.8
Creze, M., Bedretdinova, D., Soubeyrand, M., Rocher, L., Gennisson, J. L., Gagey, O., Maitre, X., & Bellin, M. F. (2019). Posture-related stiffness mapping of paraspinal muscles. J Anat, 234(6), 787-799. doi.org/10.1111/joa.12978
Huang, C. C., Jaw, F. S., & Young, Y. H. (2022). Radiological and functional assessment in patients with lumbar spinal stenosis. BMC Musculoskelet Disord, 23(1), 137. doi.org/10.1186/s12891-022-05053-x
Mielenz, T. J., Carey, T. S., Dyrek, D. A., Harris, B. A., Garrett, J. M., & Darter, J. D. (1997). Physical therapy utilization by patients with acute low back pain. Phys Ther, 77(10), 1040-1051. doi.org/10.1093/ptj/77.10.1040
Norris, C., & Matthews, M. (2008). The role of an integrated back stability program in patients with chronic low back pain. Complement Ther Clin Pract, 14(4), 255-263. doi.org/10.1016/j.ctcp.2008.06.001
Tamartash, H., & Bahrpeyma, F. (2022). Evaluation of Lumbar Myofascial Release Effects on Lumbar Flexion Angle and Pelvic Inclination Angle in Patients with Non-Specific Low Back Pain. Int J Ther Massage Bodywork, 15(1), 15-22. doi.org/10.3822/ijtmb.v15i1.709