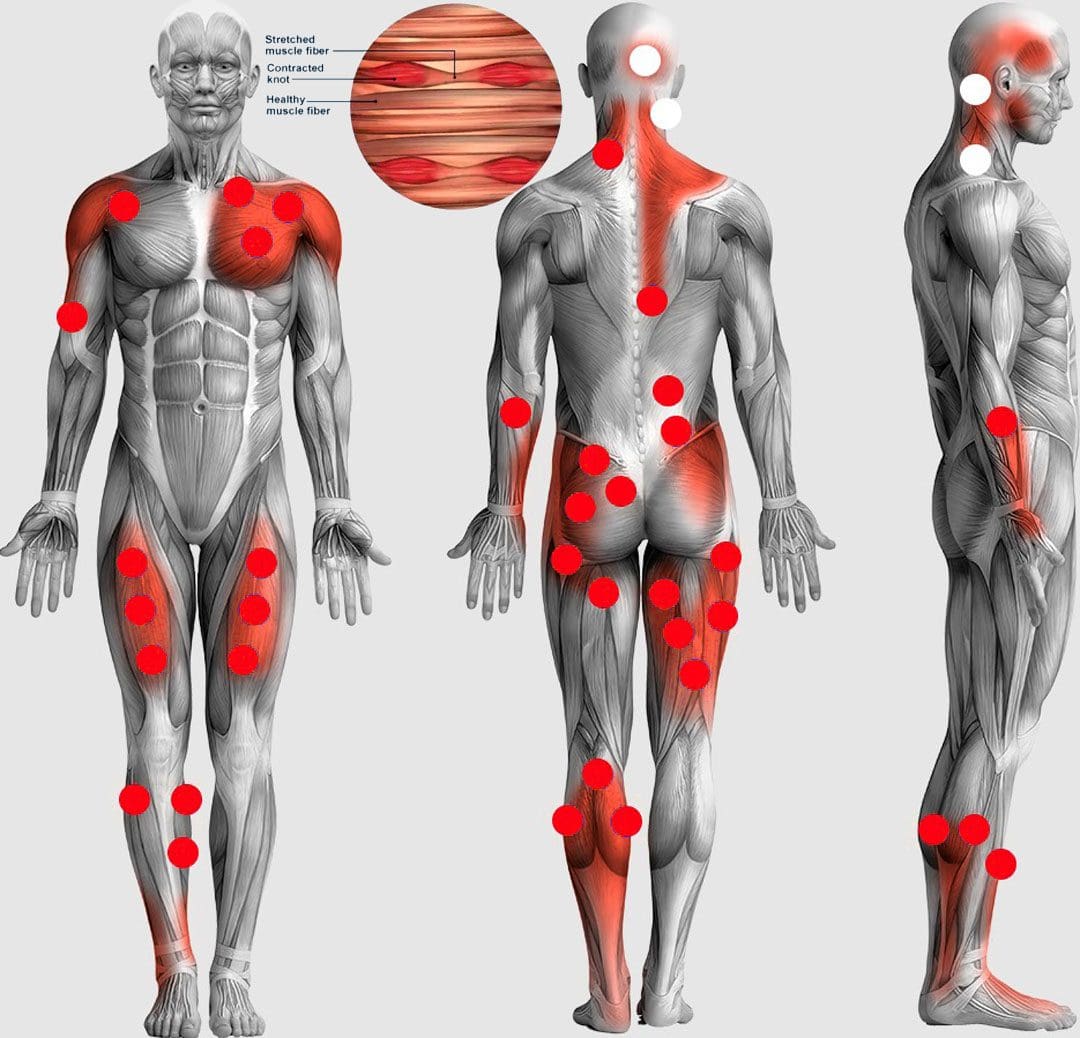
Muscle knots or trigger points are tissues/segments of muscle fibers stuck in a contracted state and balled up or become entangled. To the touch, they can feel like small bumps, nodules, or knots. They are primarily found in muscles, but they can also be found in tendons, fascia, periosteum, and ligaments. Tight muscles can limit flexibility, increase discomfort and pain symptoms, and cause further injury that can develop into chronic conditions. Trigger points can develop in all muscles and multiple muscles simultaneously. The Injury Medical Chiropractic and Functional Medicine Team can create a personalized treatment plan for trigger point alleviation.
Muscle Knots Trigger Points
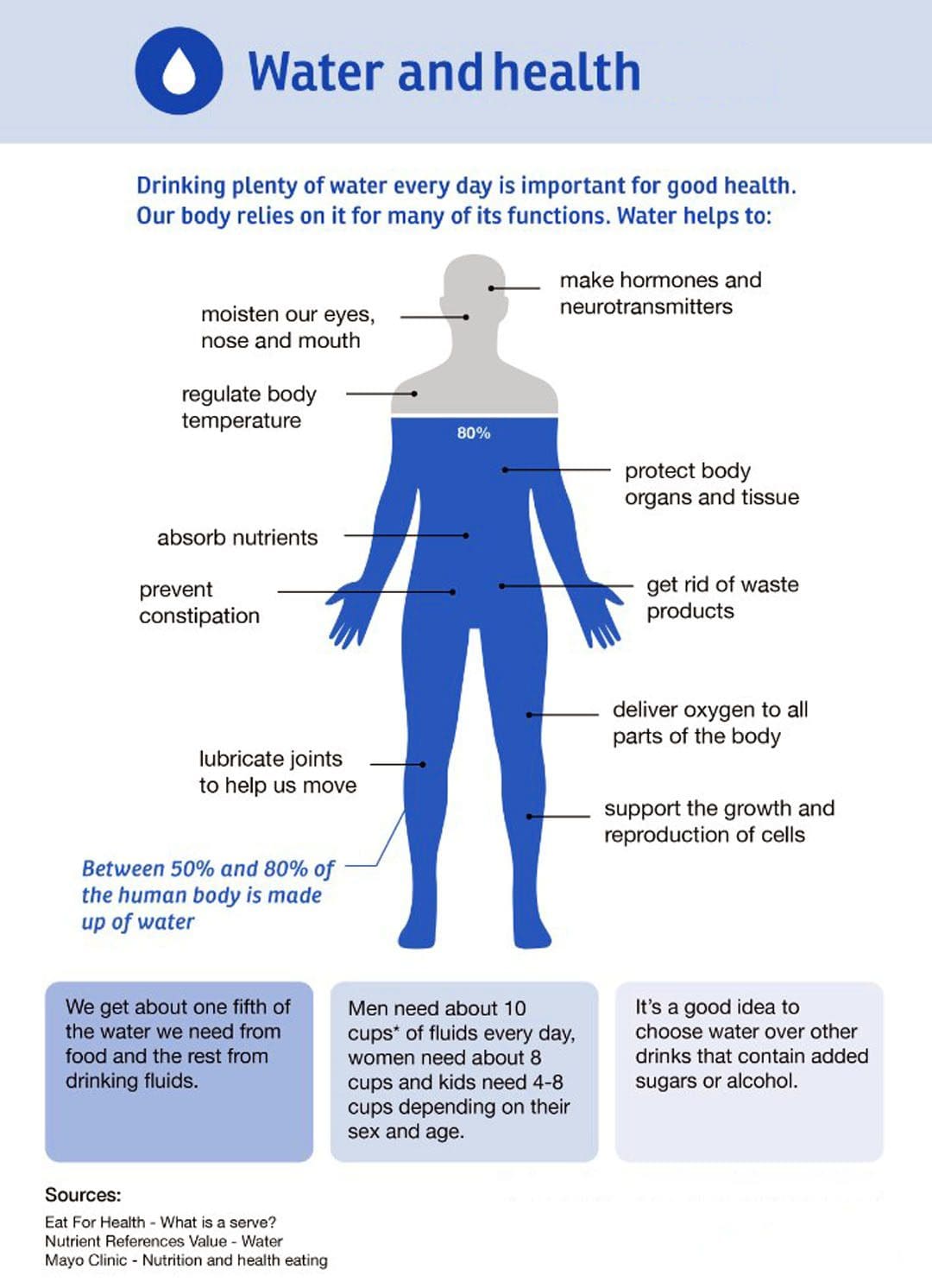
When muscle fibers are stuck in contraction, blood circulation decreases in and around the affected area, and the necessary nutrients and oxygen cannot be delivered. The excessive accumulation of the chemicals – acetylcholine, and calcium leads to a lack of oxygen in the area, which causes muscle fiber contraction and spasms. As the muscle fibers overly contract, they form a knot. Waste materials build up in the fibers as the blocked circulation doesn’t allow removal. This irritates the trigger point, which reacts by sending out pain signals. The brain responds by telling the body not to use that muscle, causing the muscle to tighten, become weak, and lose range of motion. The other muscles have to work harder to compensate.
Trigger Point Types
Active and Latent
- One type is an active trigger point.
- The trigger point causes pain and discomfort even when the muscle or tissue rests.
- The other type is latent, which means that the point does not cause pain or is sometimes even noticed until pressure is applied to the point or area.
- Both types can cause secondary trigger points to form.
- They can also prevent muscles from extending, making them feel weak.
Key and Satellite
- There are also key and satellite trigger points.
- Key trigger points activate satellite trigger points.
- Because key trigger point muscles are weakened, the muscles around that point need to work harder, causing multiple knots to form.
- Referred pain happens when a satellite trigger point causes sensations in a different area from the point itself.
Causes
The main causes include the following:
Direct Trauma
- Muscle trauma or injury can cause fibers not to heal properly, causing segments to stay deprived of oxygen and knotted.
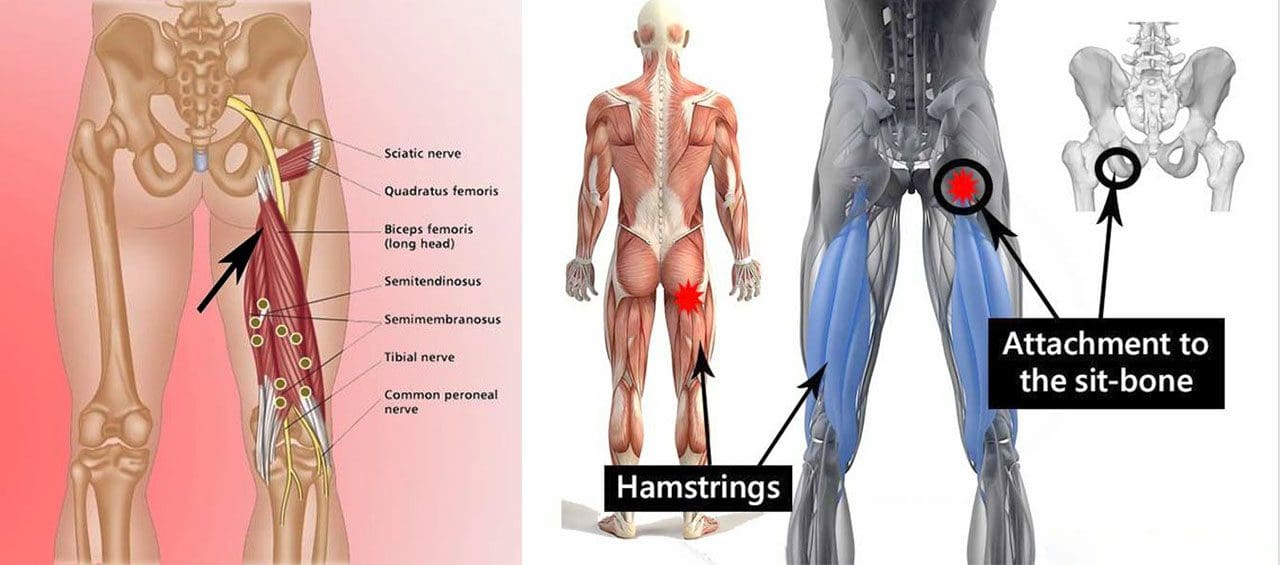
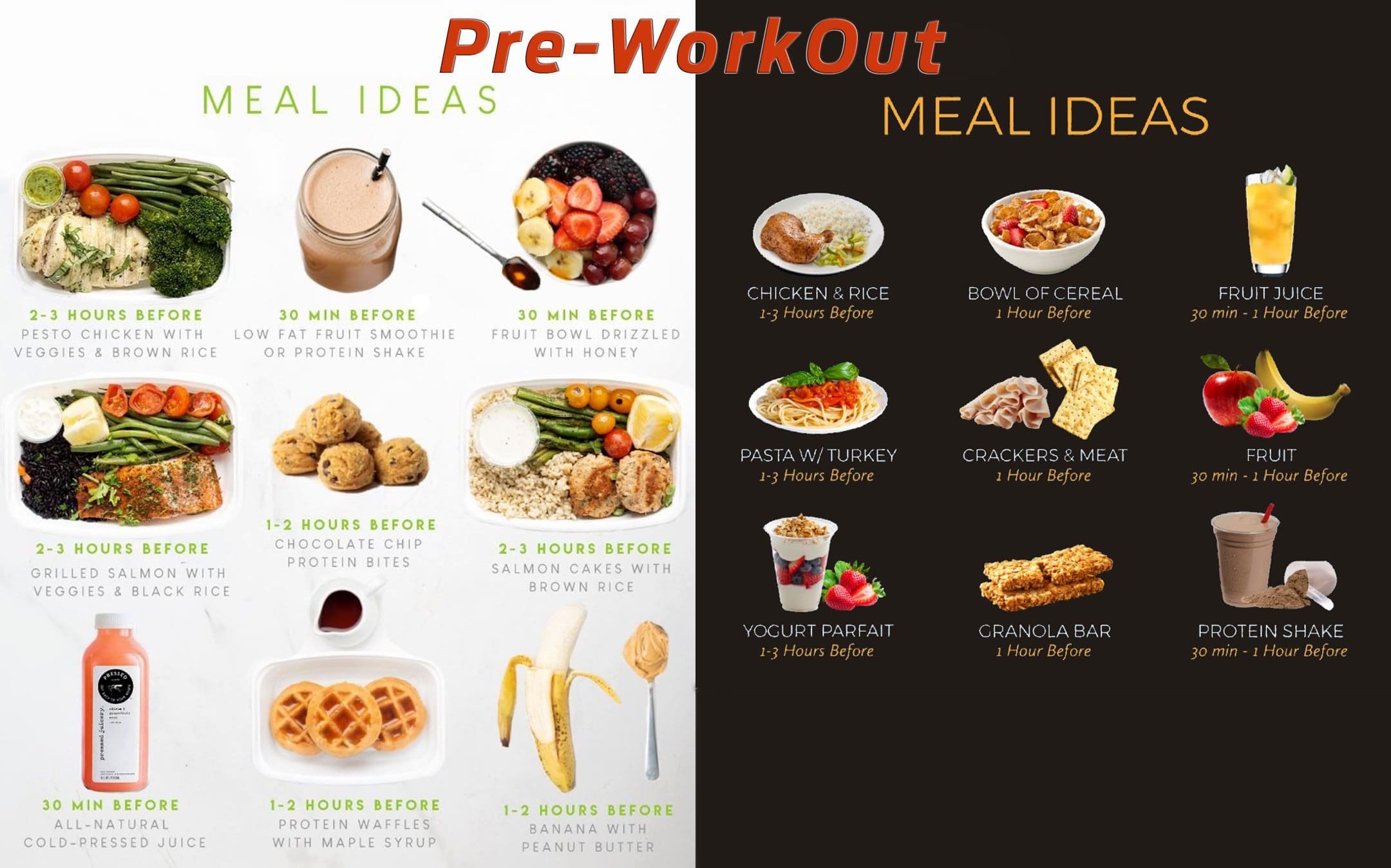
Excessive and Extended Exercising
- During exercise/physical activity, profound muscle strain and injury can occur from pushing too hard for too long without proper recovery and repair.
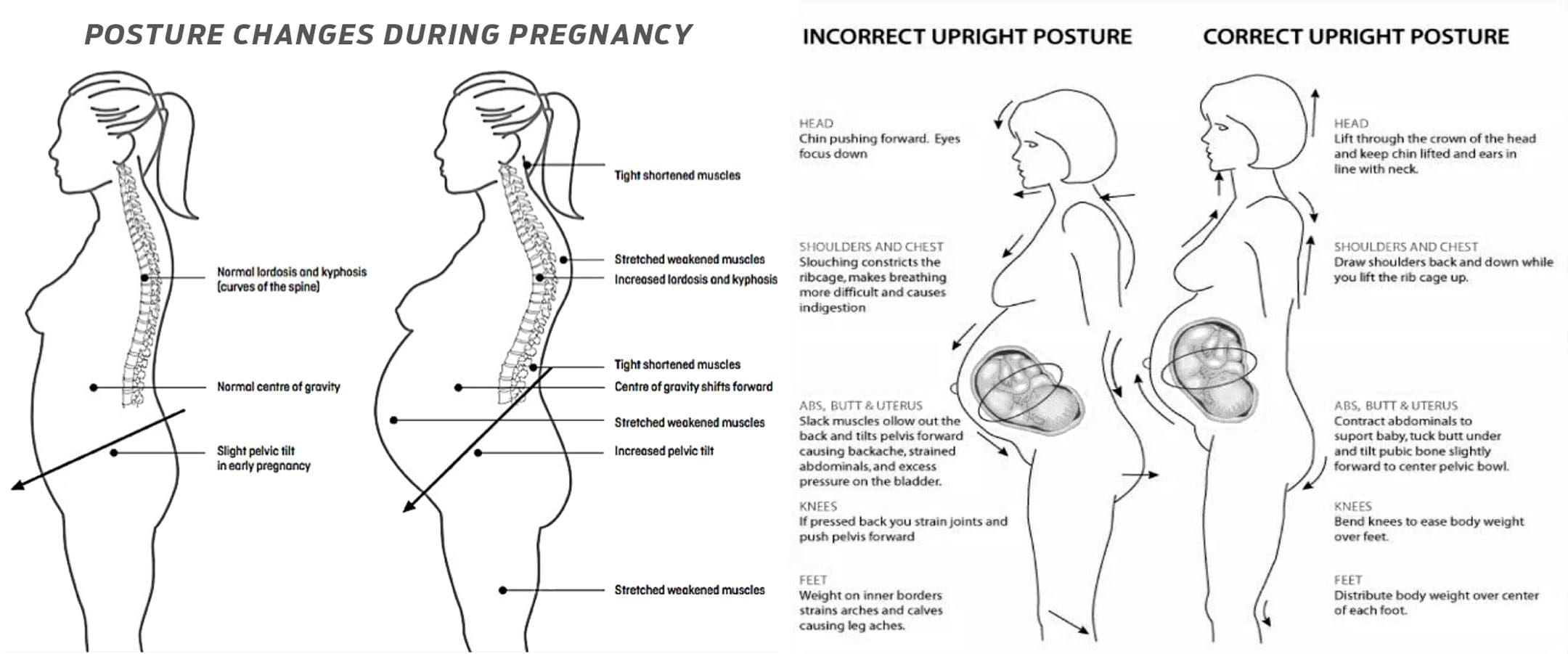
Maintaining Healthy Posture
- Unhealthy postures can cause tension, stiffness, and aches and pains.
Stress and Fatigue
- Emotional and physical stress takes a toll on the body, which can result in excessive muscle contraction.
- Most of the time, it happens subconsciously without realizing that the body is tensing up.
- This is why engaging in relaxation activities, including therapeutic massage, is important.
Inactivity
- Lack of physical activity and a sedentary lifestyle can cause muscle spasms and over-contracting, leading to muscle knots.
Medical Conditions
- Conditions that affect muscles, like arthritis and fibromyalgia or medications, can cause muscle spasms and the development of trigger points.
Chiropractic and Massage Therapy
Chiropractic and therapeutic massage is an effective treatment to relieve muscle knots and symptoms and restore the body to optimal function. Massage uses various techniques to increase blood circulation, break down inflexible scar tissue and stretch and loosen muscles. Pain and discomfort decrease by allowing the muscles to move and restoring blood flow.
Massage Therapy Chiropractic Care
References
Barbero, Marco, et al. “Myofascial pain syndrome and trigger points: evaluation and treatment in patients with musculoskeletal pain.” Current Opinion in Supportive and palliative care vol. 13,3 (2019): 270-276. doi:10.1097/SPC.0000000000000445
Cheung, Karoline, et al. “Delayed onset muscle soreness: treatment strategies and performance factors.” Sports medicine (Auckland, N.Z.) vol. 33,2 (2003): 145-64. doi:10.2165/00007256-200333020-00005
Money, Sarah. “Pathophysiology of Trigger Points in Myofascial Pain Syndrome.” Journal of Pain & palliative care pharmacotherapy vol. 31,2 (2017): 158-159. doi:10.1080/15360288.2017.1298688
Moraska, Albert F et al. “Responsiveness of Myofascial Trigger Points to Single and Multiple Trigger Point Release Massages: A Randomized, Placebo-Controlled Trial.” American Journal of physical medicine & Rehabilitation vol. 96,9 (2017): 639-645. doi:10.1097/PHM.0000000000000728
Weerapong, Pornratshanee, et al. “The mechanisms of massage and effects on performance, muscle recovery, and injury prevention.” Sports medicine (Auckland, N.Z.) vol. 35,3 (2005): 235-56. doi:10.2165/00007256-200535030-00004